
Downloaded 246 times

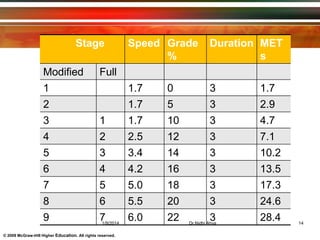
Exercise testing provides diagnostic and prognostic information by evaluating an individual's capacity during physical exertion. Common tests include treadmill tests like the Bruce Protocol and submaximal tests like the 6-minute walk test. The Bruce Protocol progresses in stages of increasing speed and incline every 3 minutes on a treadmill to induce maximum exertion. The 6-minute walk test measures how far a patient can quickly walk on a flat, hard surface in 6 minutes to assess functional capacity. Both tests monitor vital signs and symptoms to evaluate cardiovascular and pulmonary function and identify abnormalities during exercise.








![Neurophysiological facilitation of respiration [npf]](https://cdn.slidesharecdn.com/ss_thumbnails/neurophysiologicalfacilitationofrespirationnpf-180714163516-thumbnail.jpg?width=640&height=640&fit=bounds)











































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


