Download to read offline
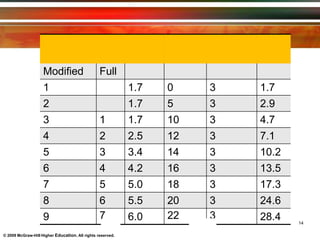
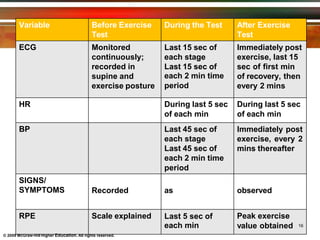

Exercise testing involves measuring an individual's physiological response to exercise in order to evaluate cardiovascular and respiratory function. There are maximal and submaximal tests, with maximal tests directly measuring VO2 max and submaximal tests estimating functional capacity. The Bruce protocol is a common maximal treadmill test that progressively increases speed and incline over stages. The six-minute walk test is a submaximal test measuring distance walked over six minutes to assess functional exercise ability.































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)













