





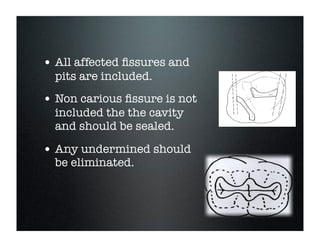
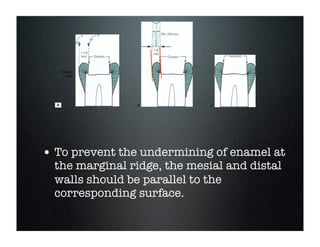















This document provides information on preparing class I amalgam cavity restorations. It discusses the materials used for amalgam fillings, including their advantages and disadvantages. It describes the Black system for cavity preparation, which involves establishing an outline, resistance, retention, and convenience form. It provides details on preparing simple, compound, and complex class I cavities, including removing caries, obtaining the proper depth and angles, and finishing cavity walls. Enameloplasty and cusp capping techniques are also covered. The goal is to conserve tooth structure while ensuring the restoration is retained and can withstand occlusal forces.
































































































