


![Sewerin’s Classification
[ 1971 ]
CLASSIFICATION
Merko et al’s Classification
[ 1974 ]
Papilla – Penetrating Frenal
AttachmentPapillary Frenal Attachment
Mucosal Frenal Attachment Gingival Frenal Attachment
References : Sewerin I – 1997; Mirko P, Miroslav S, Lubor M - 1974
Normal Frenum Persistent Tectolabial Frenum With Appendix Frenum With Nodule
Duplication of Frenum Recess of the frenum Bifid Frenum](https://image.slidesharecdn.com/frenectomy-200320141138/85/Frenectomy-6-320.jpg)
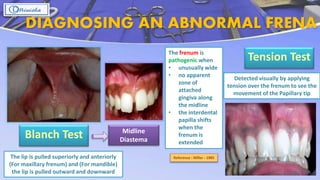
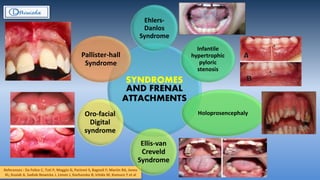
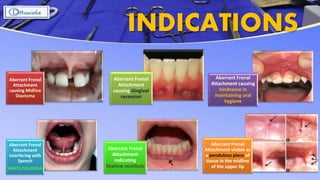

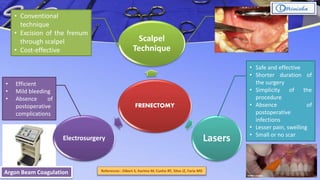
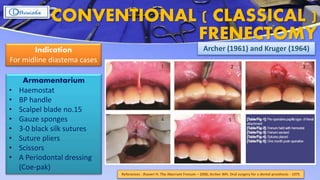



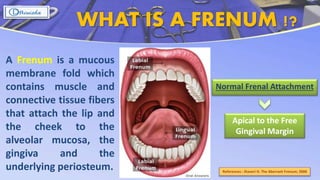
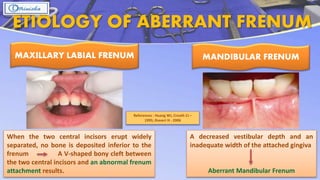
The document discusses frenectomy procedures, their classifications, and indications for correcting aberrant frena affecting oral health and aesthetics. It outlines various surgical techniques including conventional methods, electrosurgery, and laser use, as well as the criteria for diagnosing abnormal frenal attachments. It also highlights associated syndromes and complications related to frenectomy procedures.























































































