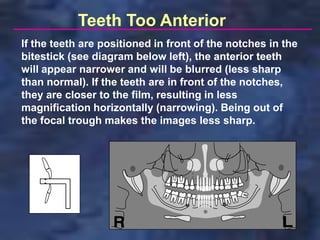
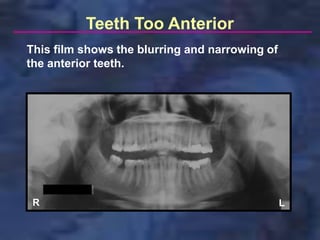
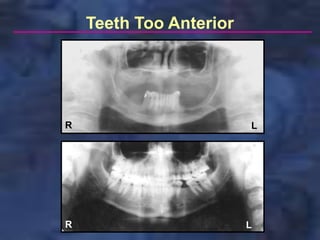
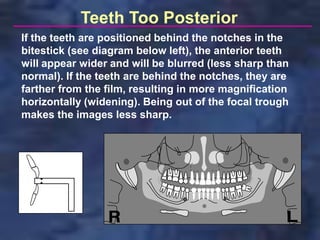
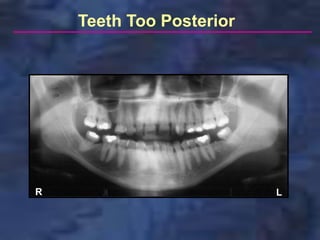
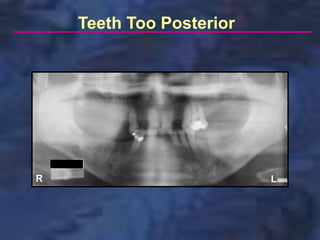
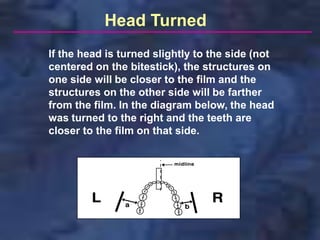
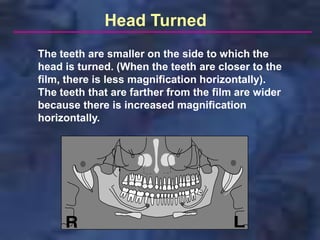
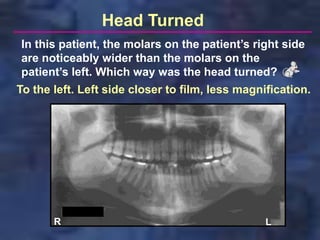
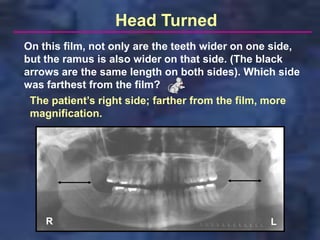
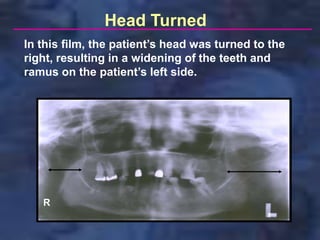
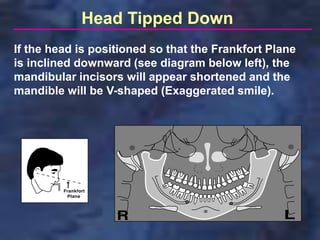

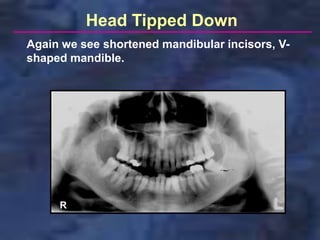
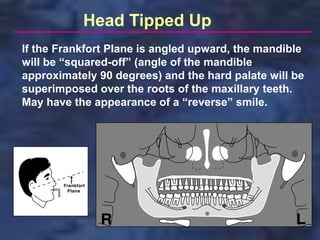
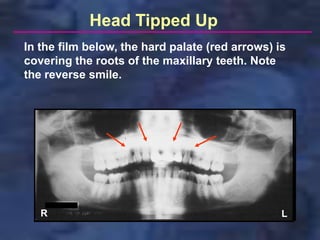
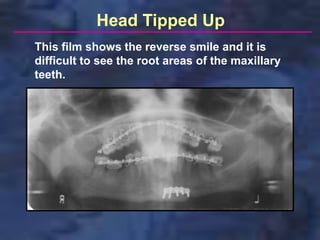
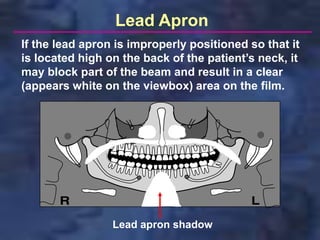
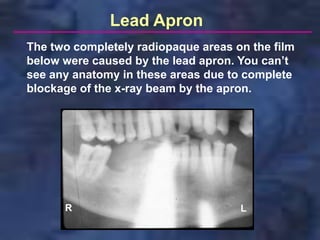

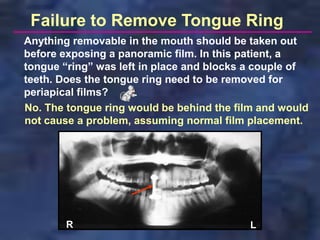
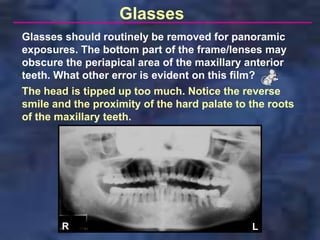
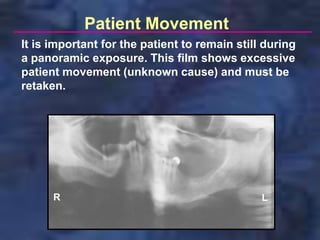
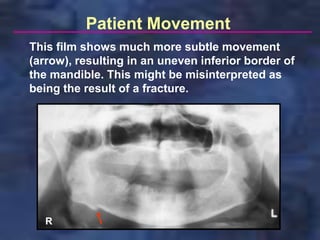
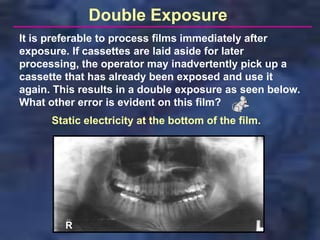
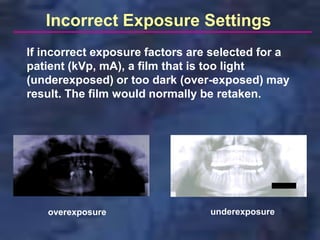

The document identifies common errors that can occur when taking panoramic dental x-rays. These include the teeth being positioned too far anterior or posterior to the focal trough, the patient's head being turned or tipped in various directions, issues with the placement of the lead apron, and other errors like patient movement, double exposures, or using incorrect exposure settings. Proper patient positioning and technique are necessary to avoid these errors and ensure diagnostic quality panoramic dental x-rays.























































































