Downloaded 33 times


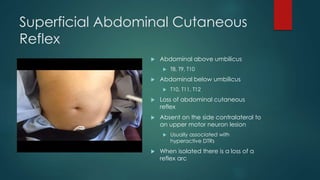
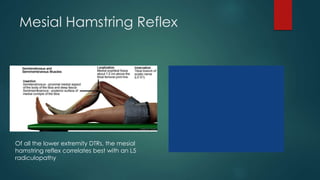

This document discusses several forgotten reflex tests including: - The ciliospinal reflex which evaluates C8-T2 nerve roots and sympathetic outflow. - The pectoral reflex which assesses C5/6 and C7/8 nerve roots via percussion of the deltopectoral groove. Hyperactivity correlates with cord lesions at C2/C3 and C3/C4. - The Hoffman reflex which assesses the C8-T1 reflex arc and is an upper motor neuron sign. - The superficial abdominal cutaneous reflex which evaluates T8-T12 nerve roots with loss indicating a loss of reflex arc. - The mesial hamstring reflex which



































































