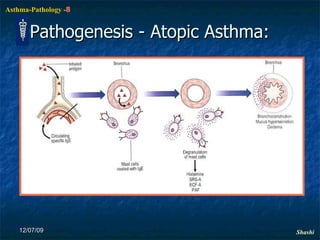
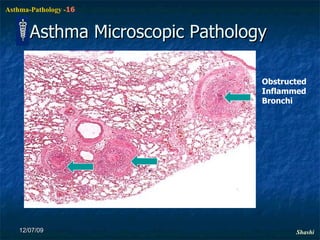
1. Asthma is a chronic inflammatory disorder of the bronchi characterized by episodic and reversible bronchospasm caused by an exaggerated response to various stimuli like allergens.
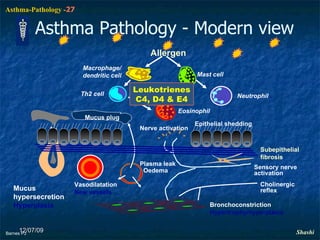
2. It affects 10% of children and 5-7% of adults worldwide. The pathogenesis involves inflammation, airflow limitation, and airway hyperresponsiveness triggered by allergens, viruses, pollutants, and other factors.
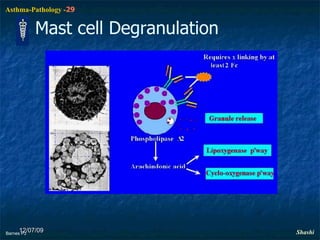
3. New understanding of the role of leukotrienes, mast cells, eosinophils and cytokines in asthma pathology has led to more targeted drug therapies that inhibit these inflammatory pathways.