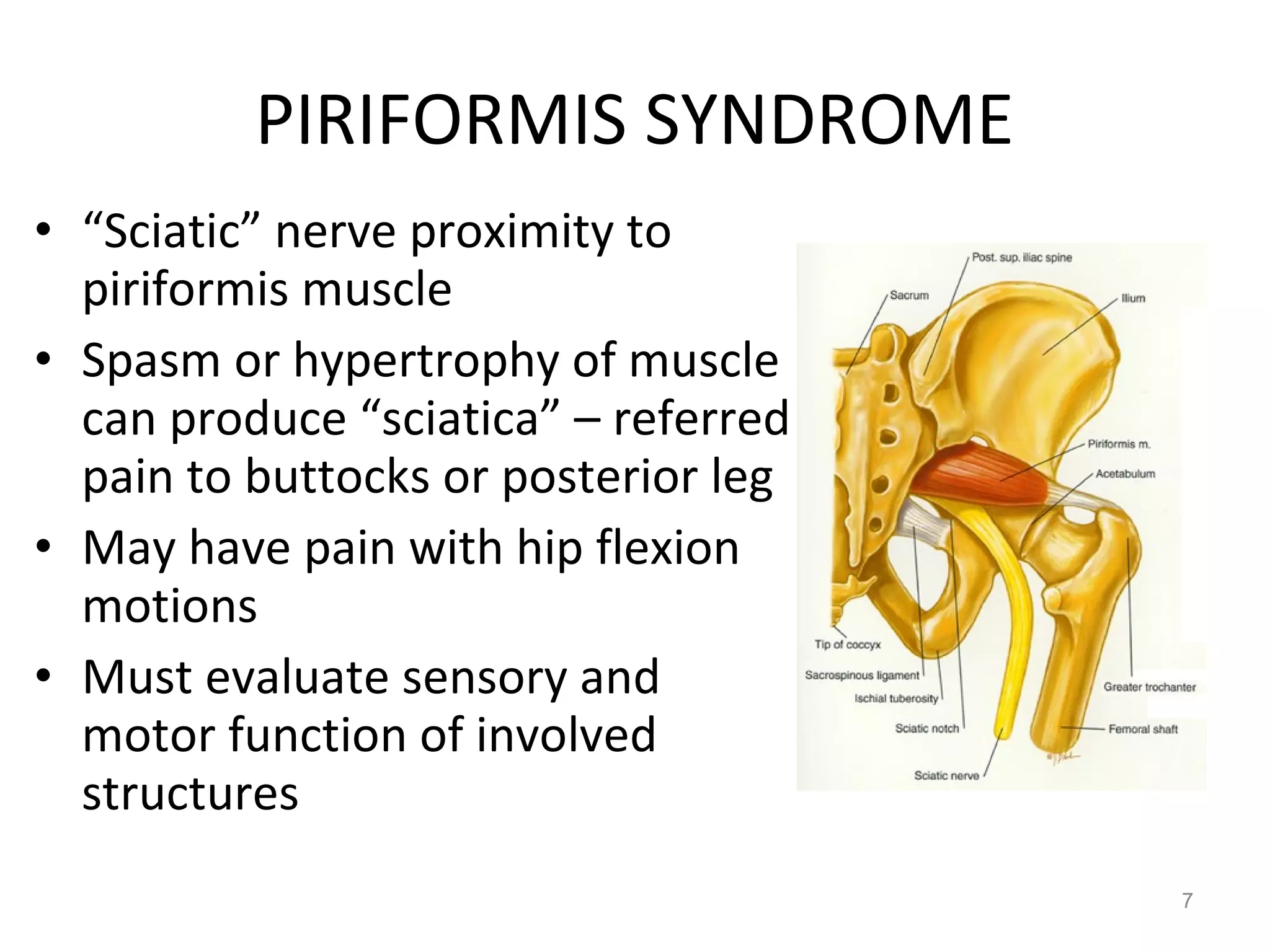
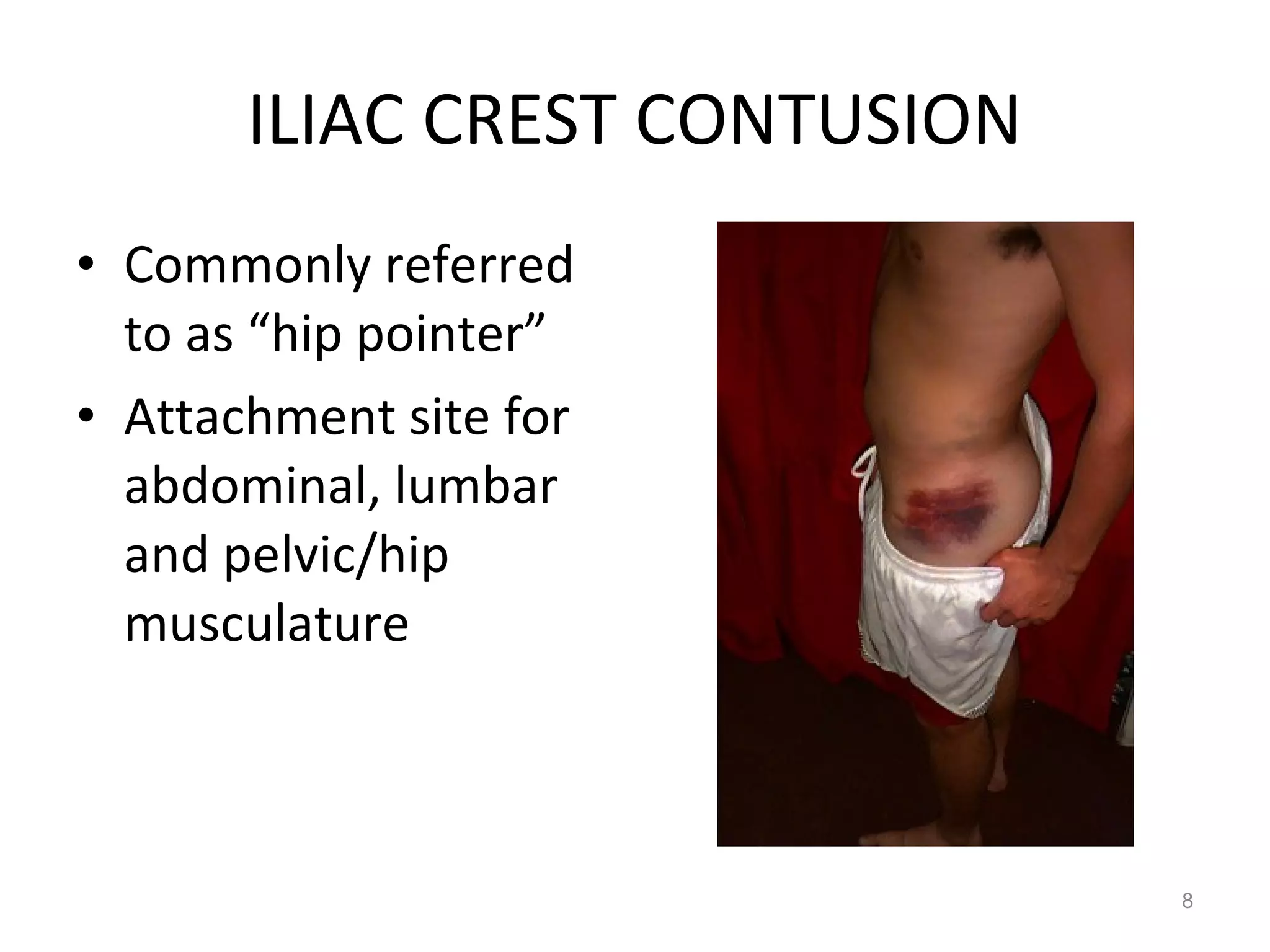
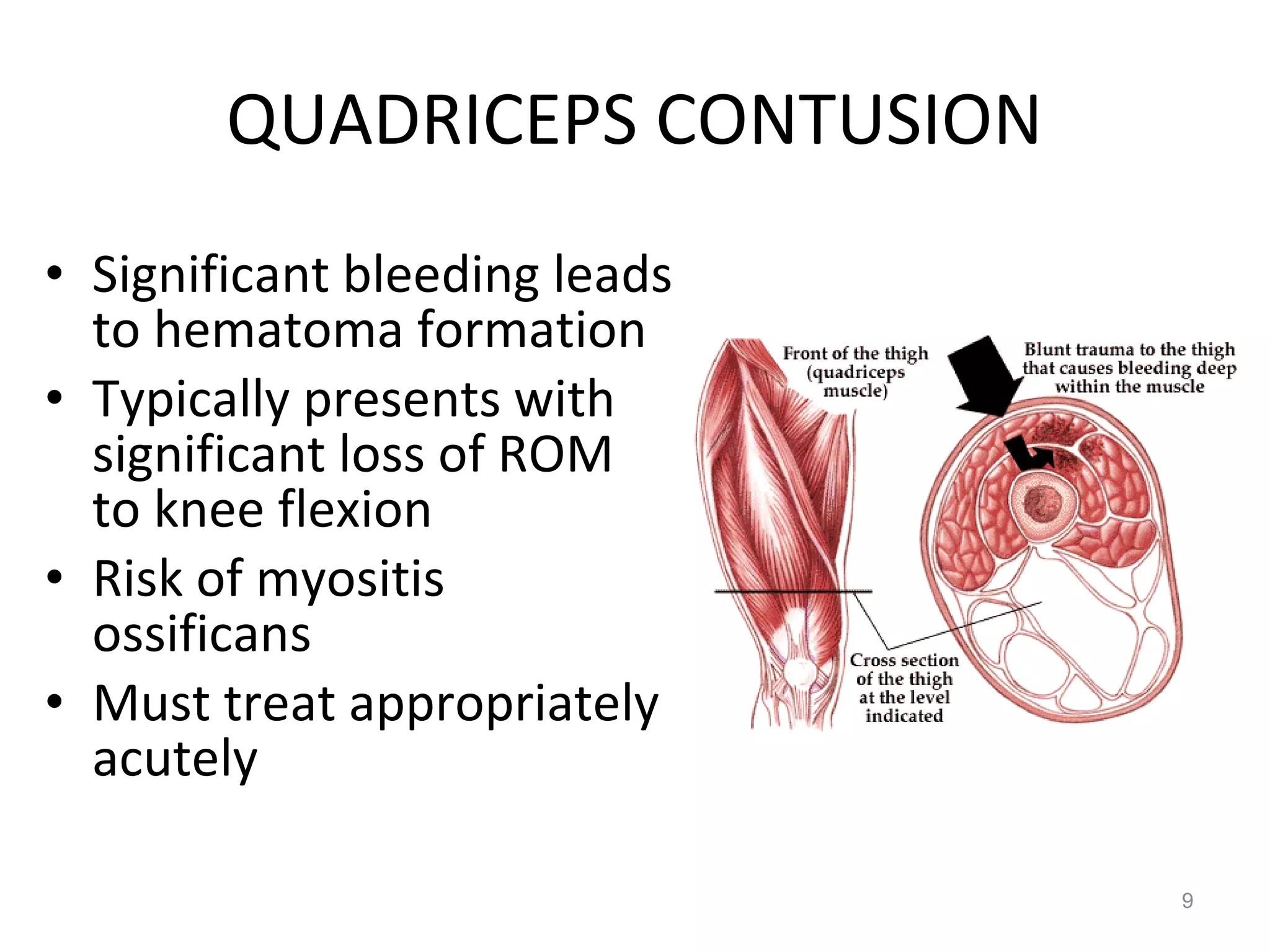
This document provides an overview of common injuries to the pelvis and thigh, including muscle strains, bursitis, degenerative hip changes, piriformis syndrome, iliac crest contusion, quadriceps contusion, hip dislocation, femur fractures and stress fractures, SI joint dysfunction, osteitis pubis, and avulsion fractures. Muscle strains typically result from eccentric contractions and present with pain at the musculotendinous junction or insertion site. Bursitis can be caused by direct trauma or repetitive friction. Degenerative hip changes develop from repetitive trauma or acute injuries. Piriformis syndrome causes referred pain that may mimic sciatica. Iliac crest contusions are commonly called "
















![Kin191 A. Ch.4. Foot. Toes. Inuries. Fall 2007[1]](https://cdn.slidesharecdn.com/ss_thumbnails/kin191a-ch-4-foot-toes-inuries-fall20071-090528145910-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)







![Hip Pointer presentation Emily and Holly[1]](https://cdn.slidesharecdn.com/ss_thumbnails/hippointer-presentationemandholly1-101124140110-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)




















































































