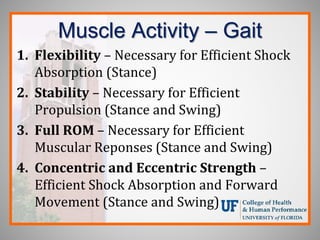
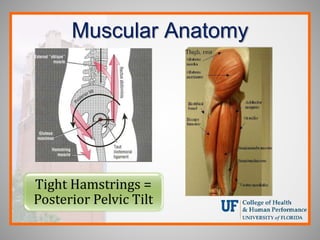
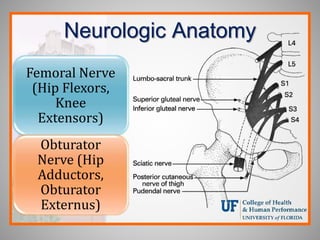
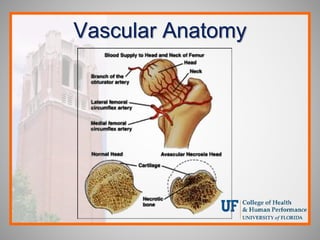
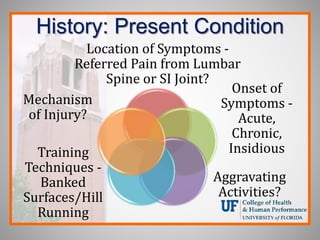
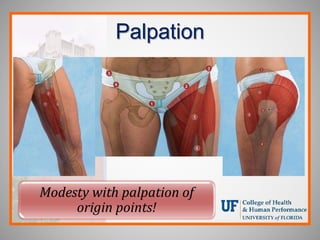
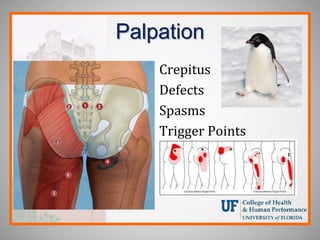
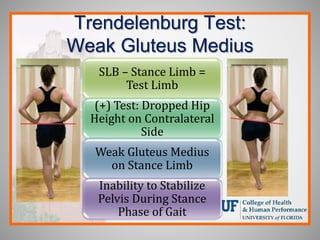
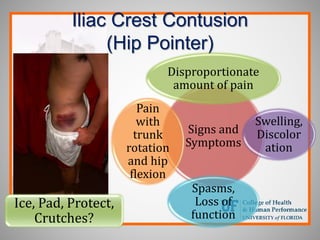
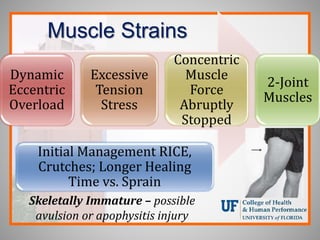
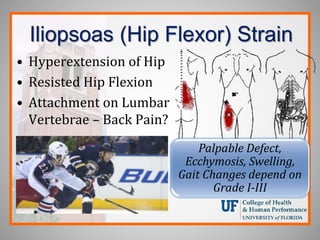
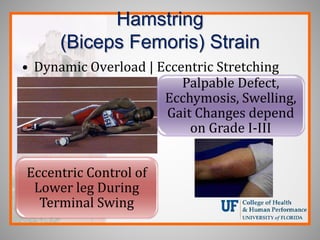
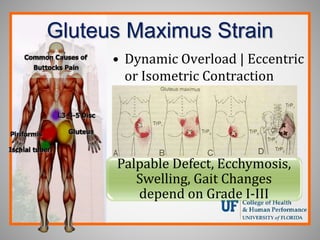
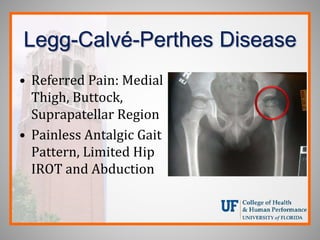
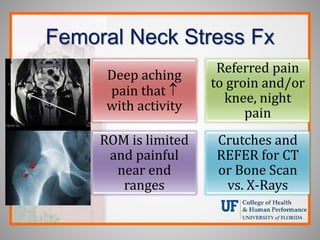
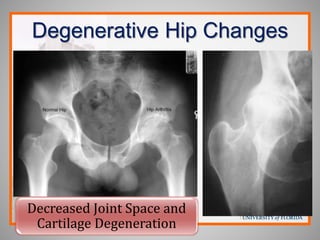
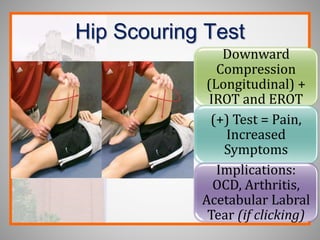
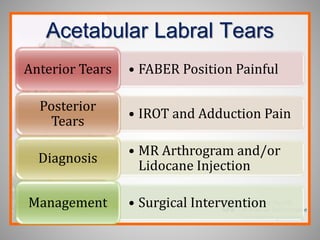
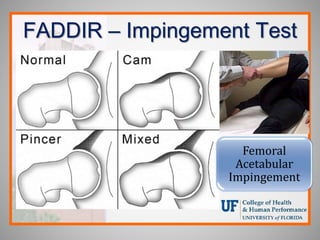
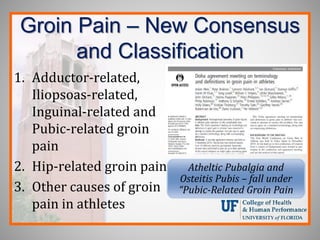
Pelvis, hip, and thigh pathologies were discussed including clinical anatomy, biomechanics, examination techniques, and common injuries seen in athletes. Key assessment tools included the Trendelenburg test, Thomas test, and FADDIR test. Common injuries addressed were muscle strains, stress fractures, Legg-Calve-Perthes disease, slipped capital femoral epiphysis, labral tears, and athletic pubalgia. Taking a systematic approach including history, inspection, palpation, special tests, and understanding biomechanics helps identify the underlying pathology.
![Key Points to Consider…
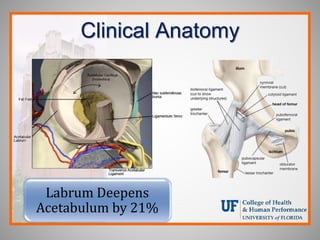
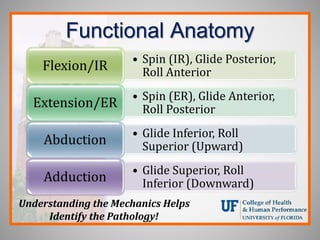
• Static and Dynamic Clinical Anatomy
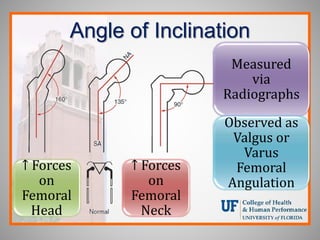
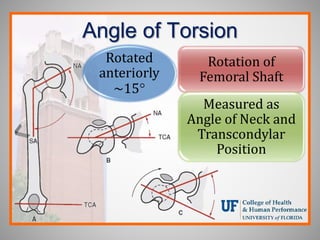
• Angle of Inclination, Angle of Torsion and
Osteo/Arthrokinematics
• Postural Screening and Observational Gait
Analysis and Core Engagement
• Kinetic Chain Linking [Hip-Pelvis Motion
Patterns CKC]
• Specialized Assessment Techniques
• Lower Quarter Screen](https://image.slidesharecdn.com/pelvishipandthighpathologies-240121173114-534098eb/85/Pelvis-Hip-and-Thigh-Pathologies-pptx-2-320.jpg)


![Structural vs. Compensatory
• Toe Out Gait Pattern – Reduced IROT at Hip
Structural
Alignment between
Femur and
Acetabulum/Pelvis
• Greater than 12°-
15° degree
Anterior
Relationship
[Anteversion]
Decreased
Anterior Femur
Head/Neck -
Condyles Alignment
• “Twisting of
Femur”
compensates for
Posterior
Femoral Head
position](https://image.slidesharecdn.com/pelvishipandthighpathologies-240121173114-534098eb/85/Pelvis-Hip-and-Thigh-Pathologies-pptx-10-320.jpg)
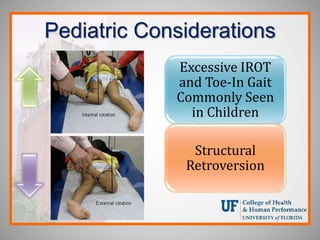
![Structural vs. Compensatory
• Toe In Gait Pattern – Reduced EROT at Hip
Structural Alignment
between Femur and
Acetabulum/Pelvis
• Less than 12°-15°
degree Anterior
Relationship
[Retroversion]
Increased Anterior
Femur Head/Neck -
Condyles Alignment
• “Twisting of
Femur”
compensates for
Anterior Femoral
Head position](https://image.slidesharecdn.com/pelvishipandthighpathologies-240121173114-534098eb/85/Pelvis-Hip-and-Thigh-Pathologies-pptx-11-320.jpg)








![Inspection
Postural
Assessment
Gait Analysis
Running Gait
Analysis
Functional
Movement
Screening
Deformity or
Defect
HP
Height
[Leg
Length,
Long-Sit
Test]
Atrophy?
Ecchymosis
Swelling](https://image.slidesharecdn.com/pelvishipandthighpathologies-240121173114-534098eb/85/Pelvis-Hip-and-Thigh-Pathologies-pptx-29-320.jpg)




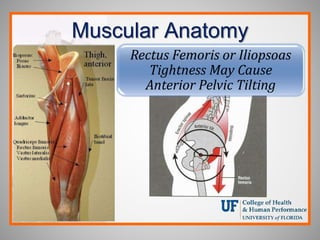
![Ely’s Test – Muscle Length
Prone Passive Knee
Flexion: (+) Test:
Hip Flexion
Implications:
Tight/Shortened
Rectus Femoris
[Anterior Pelvic
Tilting]](https://image.slidesharecdn.com/pelvishipandthighpathologies-240121173114-534098eb/85/Pelvis-Hip-and-Thigh-Pathologies-pptx-41-320.jpg)







![C-Sign and Log Roll Test
“Groin Pain” and (+) “C” Sign and Pain with
Log Roll Test [Intra-articular Pathology]](https://image.slidesharecdn.com/pelvishipandthighpathologies-240121173114-534098eb/85/Pelvis-Hip-and-Thigh-Pathologies-pptx-59-320.jpg)


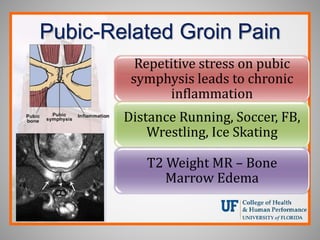
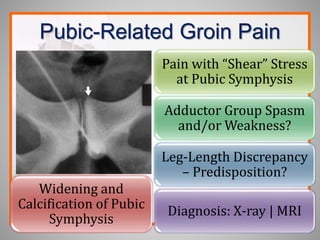
![Pubic-Related Groin Pain
MRI Referral –
Edema Pubic
Rami
Pelvic Floor
Reconstruction
Surgery [6
Weeks RTP]](https://image.slidesharecdn.com/pelvishipandthighpathologies-240121173114-534098eb/85/Pelvis-Hip-and-Thigh-Pathologies-pptx-65-320.jpg)

![FABER with Extension/IR
Moving from a FABER position into Extension
and IROT – Snapping Hip of Iliopsoas
[Lesser Trochanter]](https://image.slidesharecdn.com/pelvishipandthighpathologies-240121173114-534098eb/85/Pelvis-Hip-and-Thigh-Pathologies-pptx-71-320.jpg)