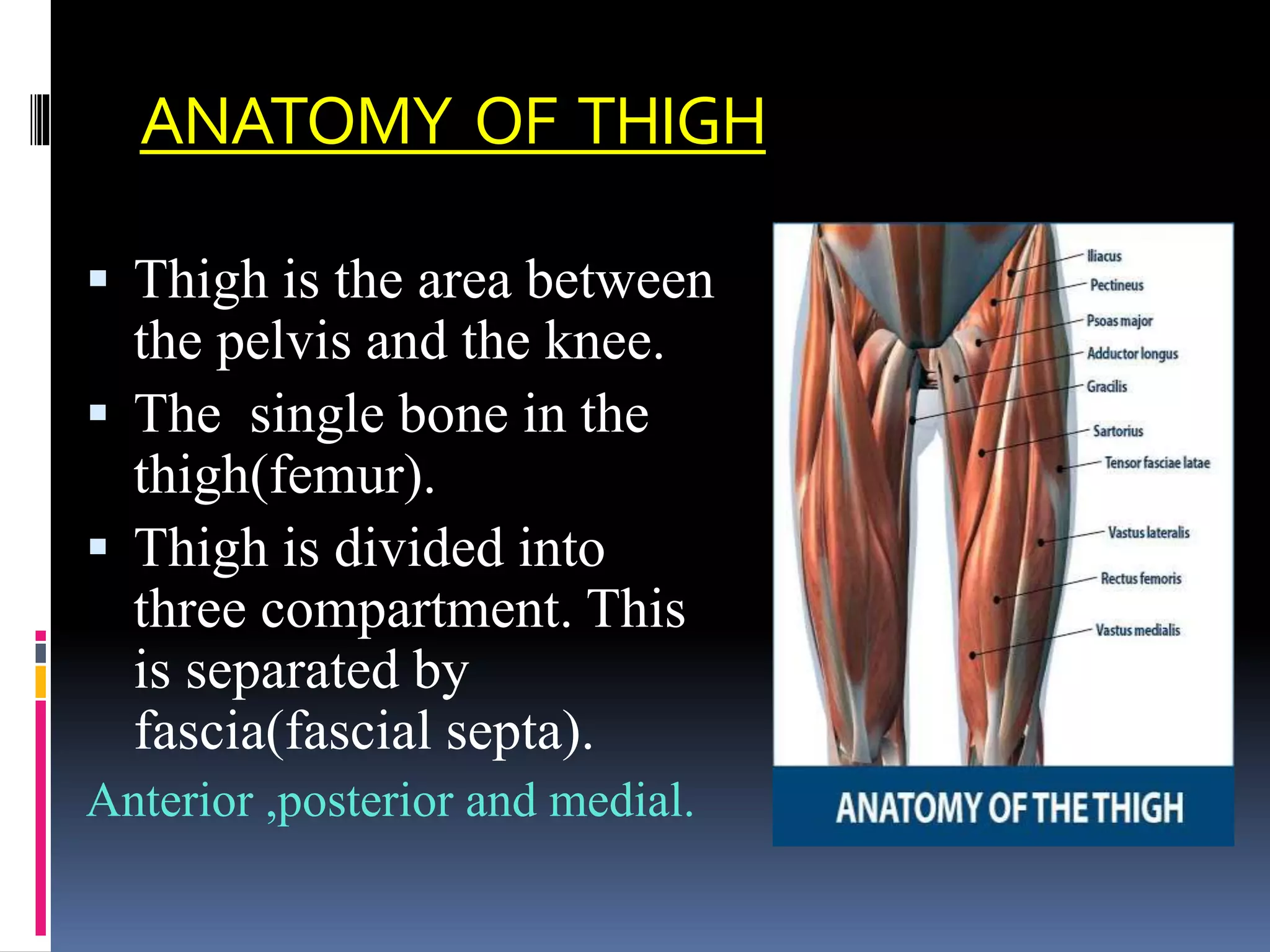
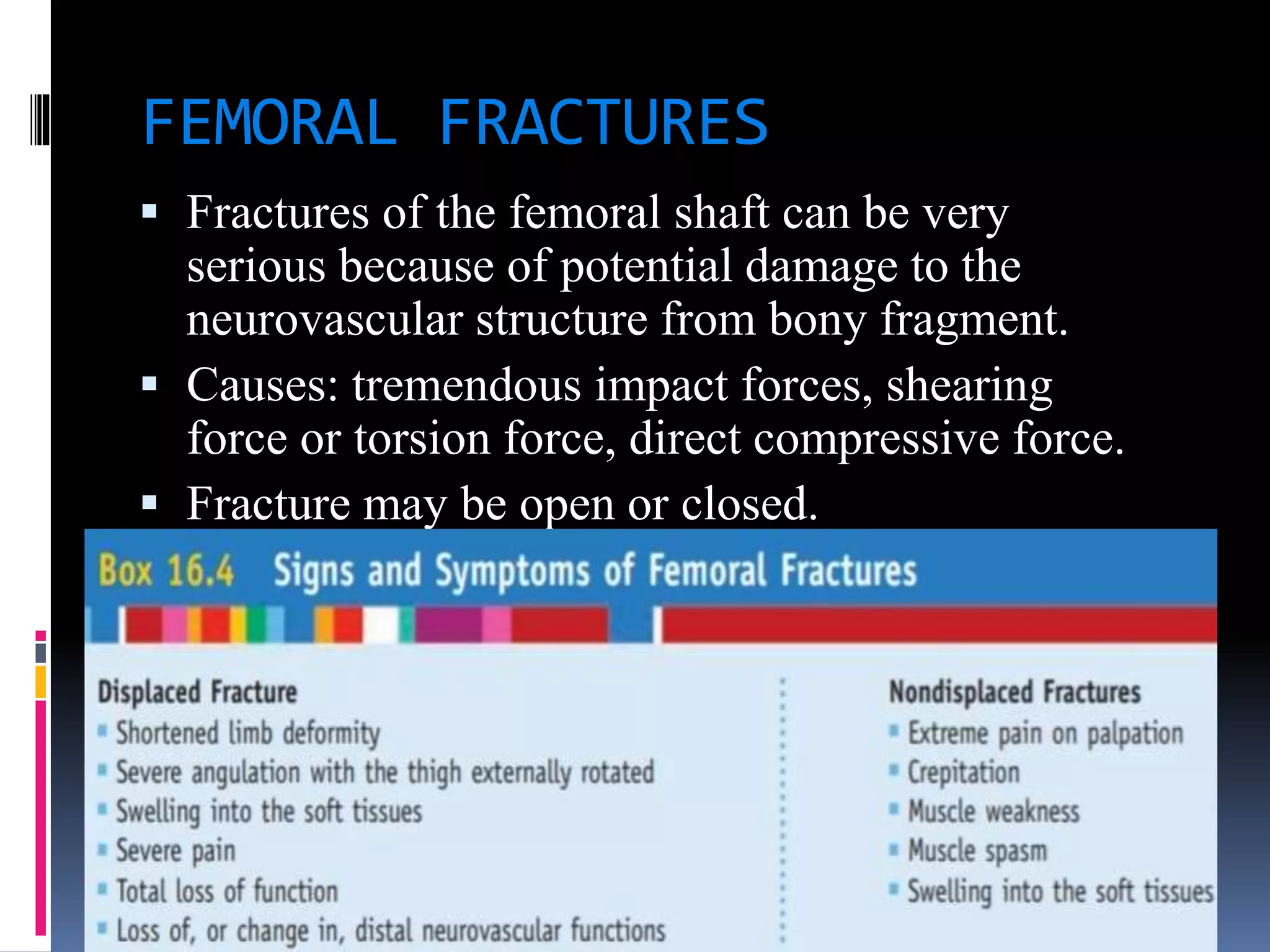
The document outlines the anatomy of the thigh, detailing its compartments (anterior, medial, and posterior) along with the muscles, innervation, and actions associated with each. It discusses common injuries such as contusions, strains, and stress fractures, including their mechanisms, symptoms, and implications for rehabilitation. Additionally, it lists special tests and measurement techniques for assessing thigh injuries.