


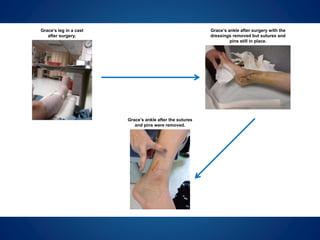

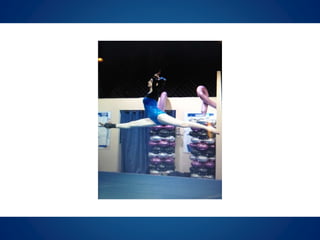

Grace dislocated and fractured her ankle at age 10 during gymnastics which required surgery and healing. At age 12, a bony bridge had developed in her growth plate requiring another surgery. Follow up showed her ankle was bowing outward and the range of motion was decreasing. Surgery was performed to remove the lateral and medial growth plates to prevent further issues. Four months post-op, her leg and ankle appeared normal and she was able to return to gymnastics with ongoing therapy. The case demonstrates how minimally invasive procedures can resolve issues and allow kids to return quickly to their activities.