Downloaded 67 times







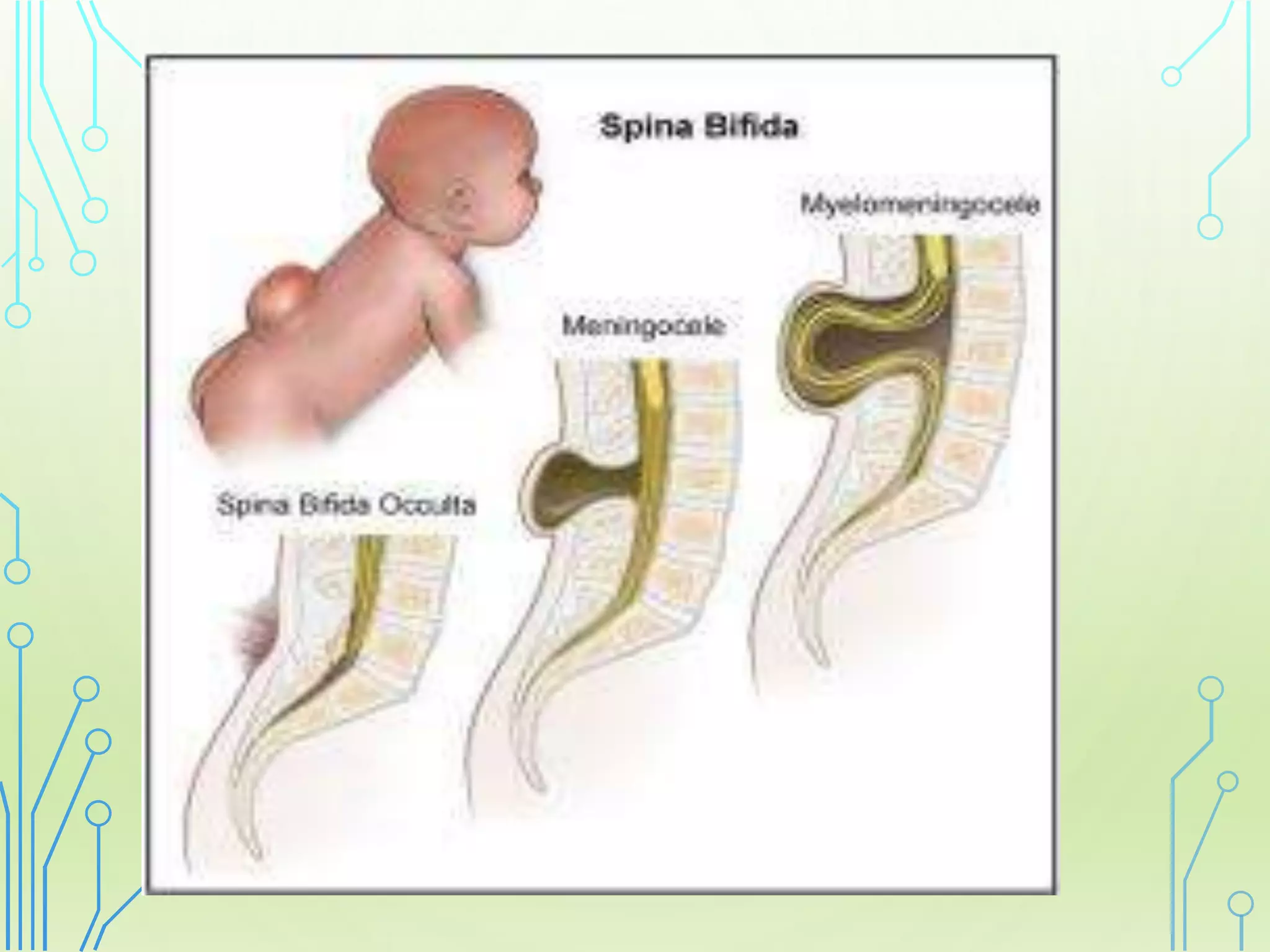










This document provides an overview of neural tube defects (NTDs), which are among the most common birth defects. It discusses the embryology, causes, types (including anencephaly and spina bifida), clinical presentation, diagnostic tests (such as ultrasound and MRI), and management (including prenatal surgery, medical care of newborns, and post-natal surgical repair). Key points covered include the importance of folic acid supplementation to prevent NTDs, the variety of potential genetic and environmental risk factors, and ongoing areas of research and debate around improving treatment and outcomes.




































![Neural tube defect [ntd]](https://cdn.slidesharecdn.com/ss_thumbnails/neuraltubedefectntd-170814055941-thumbnail.jpg?width=640&height=640&fit=bounds)






























