Downloaded 2,219 times



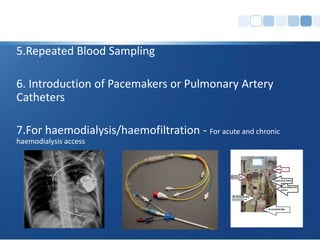




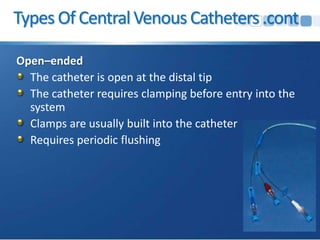
































Central venous catheters (CVCs) are intravenous devices used for patients with difficult vascular access and for administering medications, monitoring pressure, and providing nutrition. They can be categorized into non-tunneled, tunneled, PICC, and implantable ports, each with specific features and indications. Complications such as infections and pneumothorax are significant concerns, with various strategies recommended to minimize these risks.























































































