Downloaded 478 times




![The manifestations of early congenital syphilis most often occur within the first 3 to 7 weeks after birth and result from active, disseminated fetal infection and the subsequent inflammatory response. Hepatosplenomegaly/hepatitis, jaundice, lesions on the skin and/or in the mouth (Fig. 5), rhinitis, inflammation of long bones (osteochondritis, perichondritis), adenopathy, and hematologic disturbances (anemia, thrombocytopenia) are typical early manifestations of congenital syphilis. Low birth weight and failure to thrive also may occur. Necrotizing funisitis--an inflammation of the umbilical cord characterized by spiral stripes of red and blue discoloration resembling a "barber's pole"--is a specific sign of congenital syphilis.[1]](https://image.slidesharecdn.com/syphilis-1218118968233457-9/75/Syphilis-and-Neurosyphilis-101-8-2048.jpg)



![types of neurosyphilis There are four clinical types of neurosyphilis: Asymptomatic neurosyphilis Meningovascular syphilis General paresis [23] Tabes dorsalis](https://image.slidesharecdn.com/syphilis-1218118968233457-9/75/Syphilis-and-Neurosyphilis-101-12-2048.jpg)



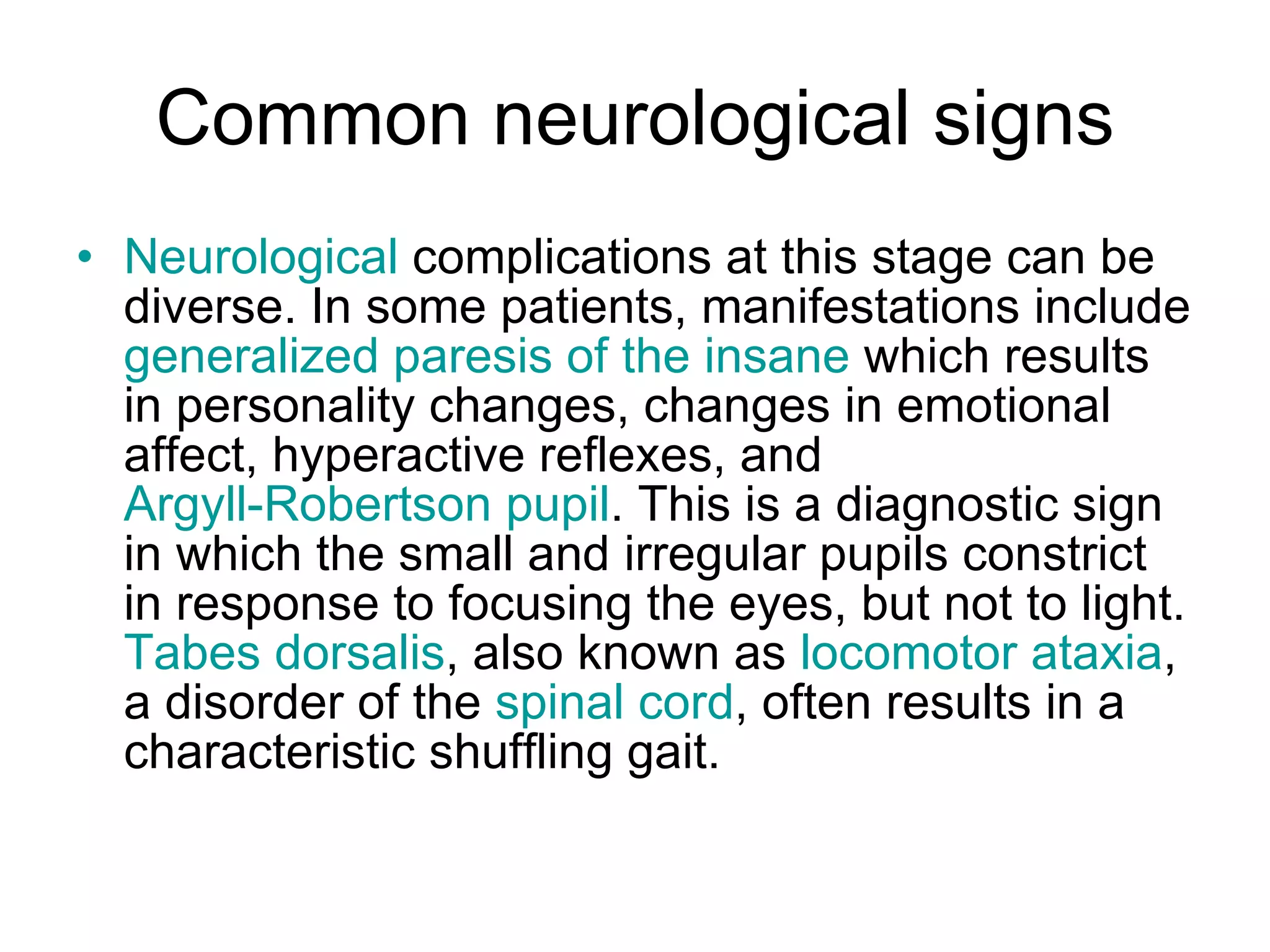







The document discusses various stages and types of syphilis including neurosyphilis. It describes the typical early manifestations of congenital syphilis in infants as well as the four clinical types of neurosyphilis - asymptomatic neurosyphilis, meningovascular syphilis, general paresis, and tabes dorsalis. General paresis is a chronic dementia that results in death within 2-3 years and is characterized by personality changes, memory loss, and poor judgment. Tabes dorsalis affects the spinal cord and can cause an unsteady gait and sensory issues. Diagnosis of neurosyphilis involves lumbar puncture, CSF analysis, and various imaging and blood tests. Treatment is with pen




















































![Neuropsychiatry [2017]](https://cdn.slidesharecdn.com/ss_thumbnails/neuropsychiatricmanifestationofcommonneurologicaldisorders-171001003940-thumbnail.jpg?width=640&height=640&fit=bounds)











































