Downloaded 1,653 times











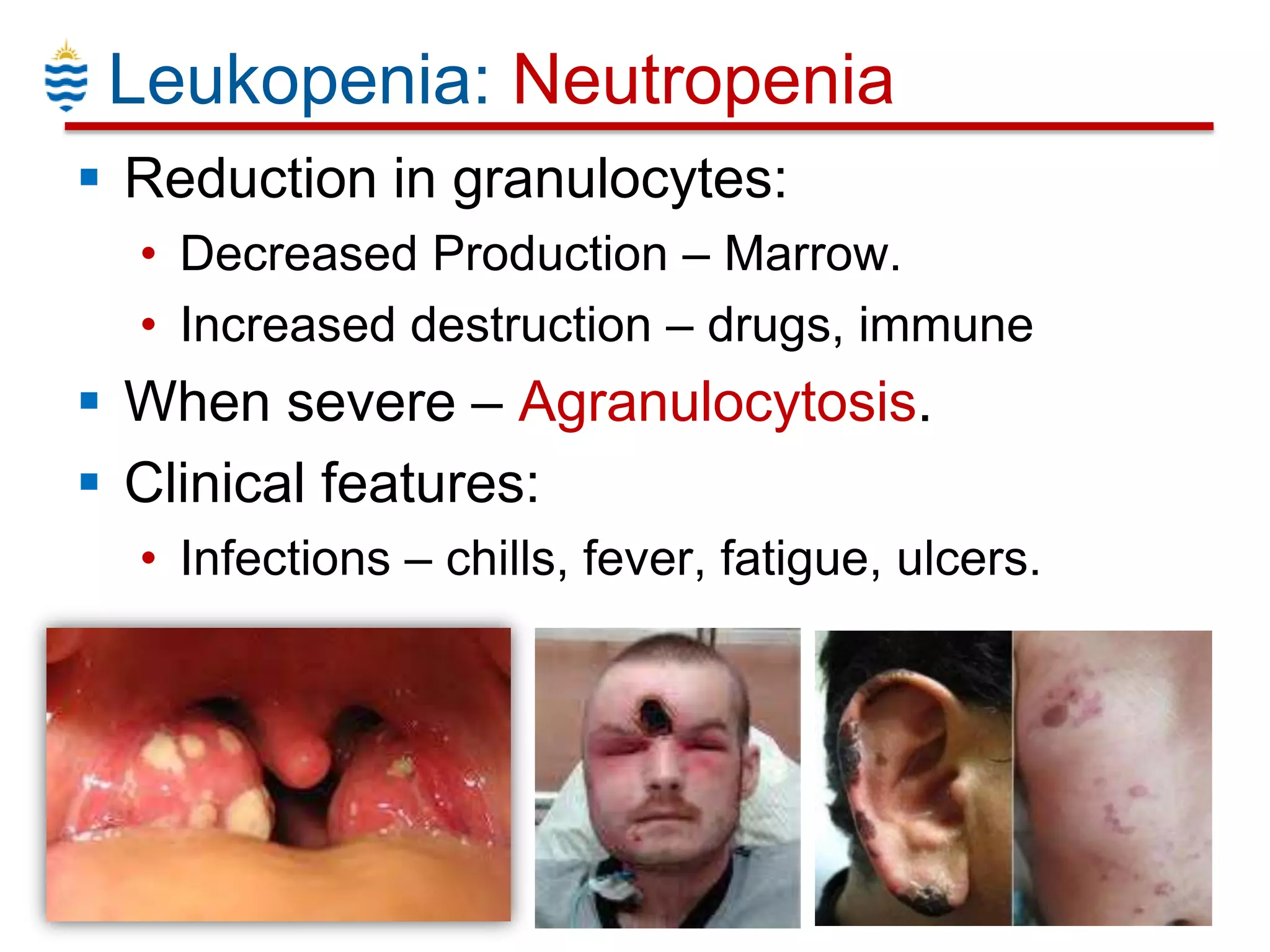


















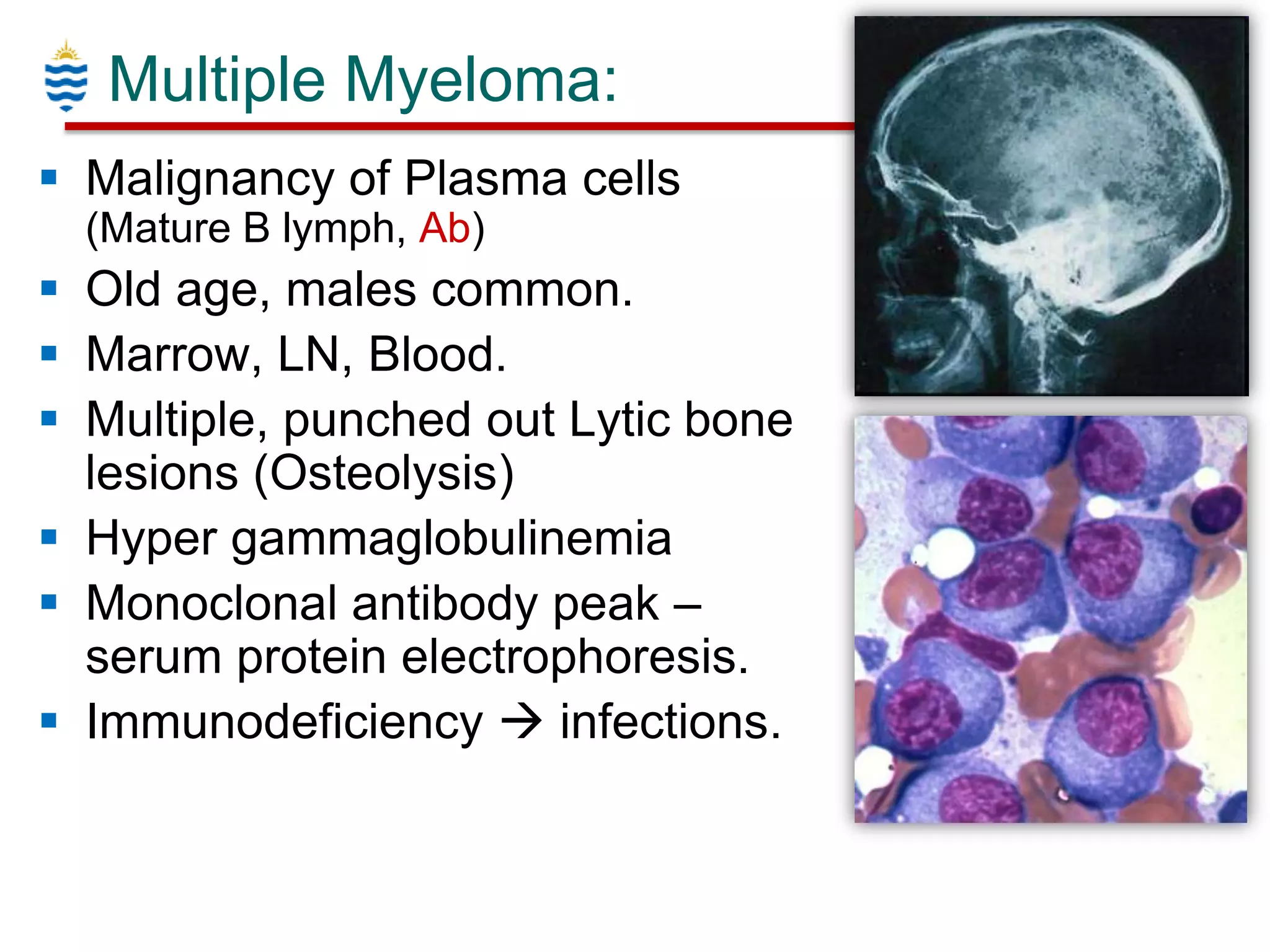







This document provides an overview of white blood cell disorders, including common conditions such as neutropenia, lymphocytosis, leukemia, and lymphoma. It begins with an introduction to normal white blood cell production and classification. Key points covered include the clinical features and pathogenesis of various leukopenias and leukocytoses. Classification systems for hematologic neoplasms such as leukemia subtypes (AML, ALL, CML, CLL) and lymphomas (Hodgkins, Non-Hodgkins) are summarized. Premalignant conditions like myeloproliferative disorders and myelodysplastic syndromes are also briefly outlined.























































































