Downloaded 26 times


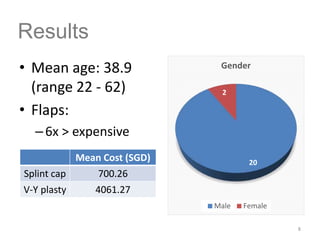
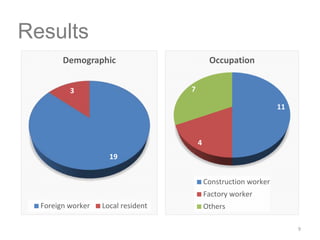
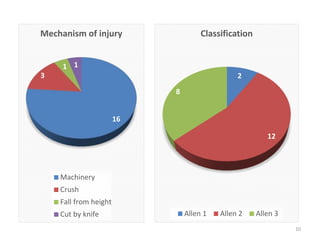
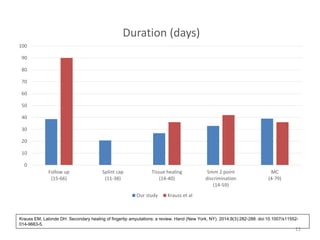



This document summarizes a study on the use of semi-occlusive dressing and splint caps for the management of fingertip amputation injuries. The study aimed to show that fingertip injuries can be treated conservatively with comparable results to surgical management like V-Y plasty. It was a prospective study of 20 patients with fingertip amputations who underwent splint cap treatment. The results found that splint caps provided a pain-free environment for healing, with outcomes comparable to surgery but at a much lower cost. Further large-scale studies are still needed to validate splint caps as a viable alternative to surgery.





















![SOFT TISSUE INJURY [Recovered].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/classificationofsofttissueinjuryrecovered-220424142623-thumbnail.jpg?width=640&height=640&fit=bounds)

































































