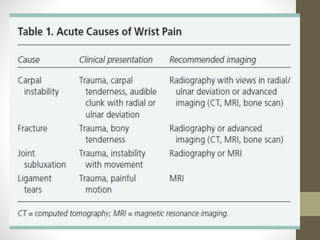
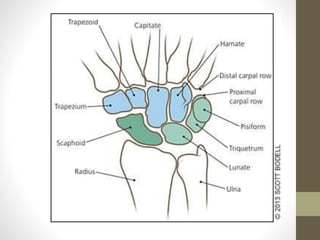
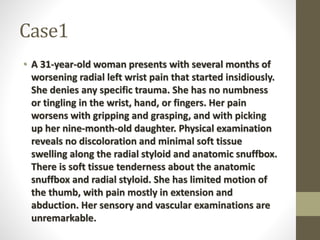
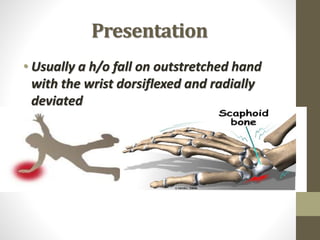
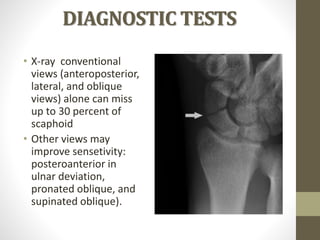
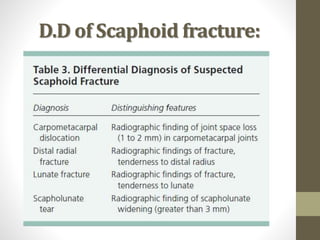
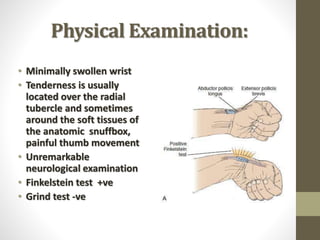
A 31-year-old woman presents with left wrist pain that worsens with gripping and picking up her daughter. Examination finds tenderness near the anatomic snuffbox and radial styloid with limited thumb motion. This is consistent with a scaphoid fracture, which presents with wrist tenderness and pain with axial pressure on the thumb and can be difficult to diagnose without advanced imaging given missed fractures on initial x-rays.
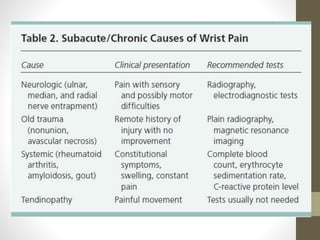
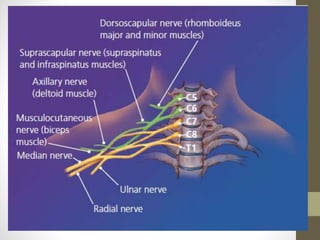
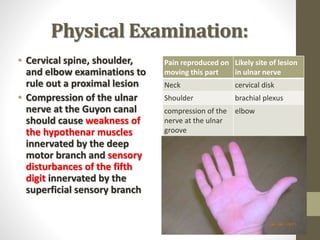
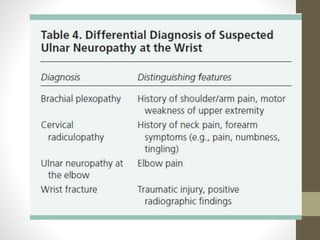
A 39-year-old woman has right wrist pain and numbness in her fifth finger. Examination reproduces tingling with tapping the pisiform. This suggests ulnar neuropathy, which causes sensory changes in the fourth and fifth digits from compression of the ulnar nerve as it








































































![Session 6 se and complications [repaired]](https://cdn.slidesharecdn.com/ss_thumbnails/session6seandcomplicationsrepaired-180404084057-thumbnail.jpg?width=640&height=640&fit=bounds)













![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)






