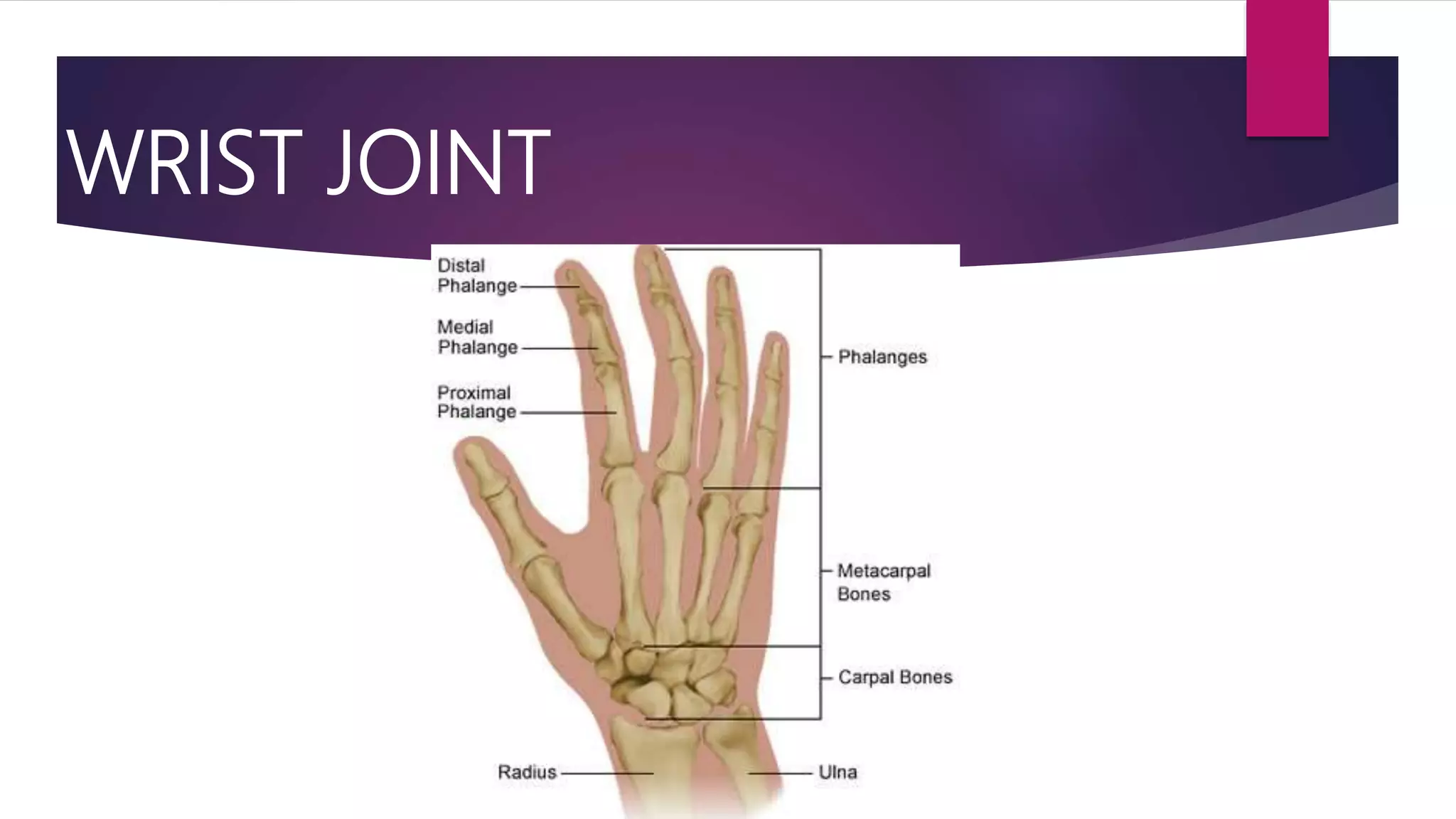
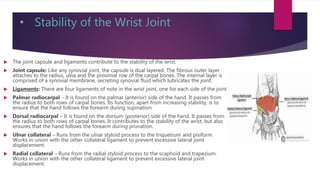
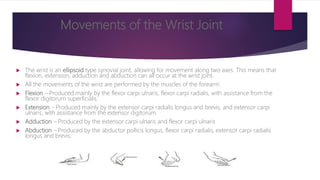
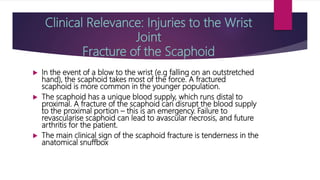
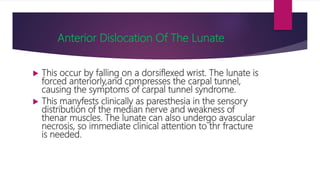
The wrist joint, or radiocarpal joint, connects the forearm to the hand. It is formed by the distal end of the radius articulating with the proximal row of carpal bones. The ulna does not directly articulate with the wrist joint. The wrist joint allows for flexion, extension, adduction and abduction through movement along two axes. Common injuries to the wrist joint include fractures of the scaphoid, anterior dislocation of the lunate, and Colles' fractures of the radius.