Downloaded 796 times

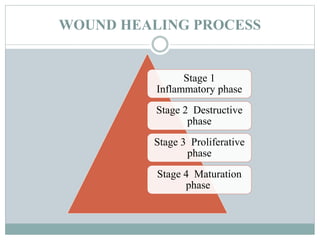


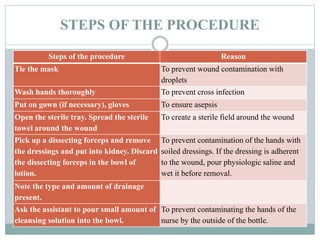






The document provides a comprehensive overview of wound care, including the definition and classification of wounds, the four stages of wound healing, and factors influencing the healing process. It details the principles and types of wound dressings, as well as step-by-step instructions on how to perform wound dressing while maintaining aseptic technique. Additionally, it emphasizes the importance of preparation and aftercare to ensure patient comfort and wound hygiene.













































![4_5933593097194704354[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/459335930971947043541-230123122719-1e0eaf18-thumbnail.jpg?width=640&height=640&fit=bounds)








































