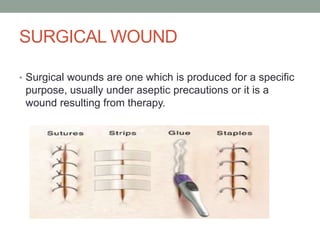
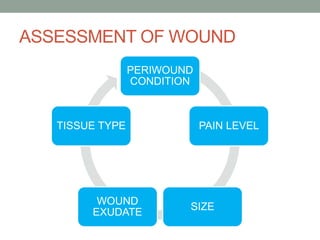
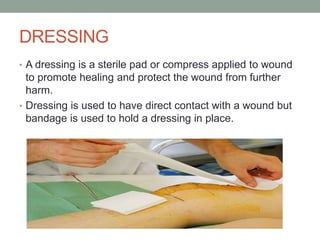
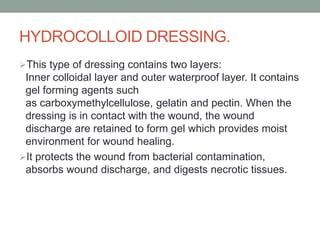
This document discusses surgical wound dressing. It defines a surgical wound and different types of dressings used including semi-permeable film, foam, hydrogel, hydrocolloid and alginate dressings. The purpose of surgical wound dressing is to prevent infection, assess healing, protect the wound and promote healing. Principles of dressing include asepsis to prevent spread of microorganisms. Preparation of the patient, environment and required articles is explained. The procedure of wound assessment, removal of soiled dressings and application of new sterile dressing is demonstrated in steps.