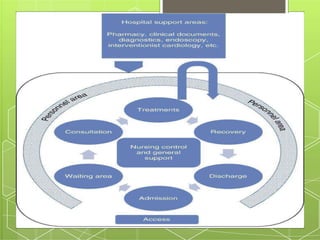
The document provides information on ward management and the patient admission and transfer process. It discusses [1] the admission checklist and procedures nurses follow when a patient is admitted, [2] the various types of hospital wards and factors considered in ward design, and [3] the equipment, orders, and level of transfer required to safely move a patient within or between facilities.