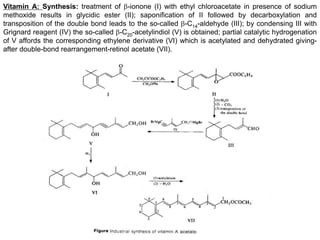
Downloaded 27 times




























Vitamins are organic compounds that are essential for normal human metabolism. They are divided into fat-soluble vitamins (A, D, E, K) and water-soluble vitamins. Deficiencies can occur due to inadequate intake, malabsorption, or other factors. Fat-soluble vitamins are stored in the body while water-soluble vitamins are not stored as much and excess is excreted. Deficiencies of specific vitamins can lead to diseases like xerophthalmia (vitamin A), rickets (vitamin D), anemia (vitamin E), or bleeding disorders (vitamin K).























































































