This document summarizes visual dysfunction in Parkinson's disease. It discusses several key points:
1) Parkinson's disease causes non-motor symptoms including various visual issues like difficulty reading, double vision, and visual hallucinations.
2) Visual problems are linked to specific motor symptoms and predict disease severity and progression.
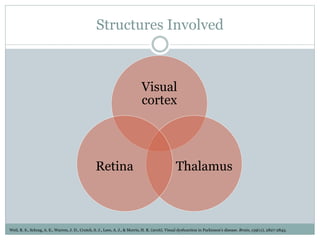
3) The neurobiology involves dopamine and other neurotransmitters affecting visual brain areas and circadian rhythms.
4) Identifying visual deficits could help diagnose Parkinson's earlier and predict outcomes like dementia.








































![Parkinson's Disease [Advanced Pharmacology]](https://cdn.slidesharecdn.com/ss_thumbnails/07-210419085948-thumbnail.jpg?width=640&height=640&fit=bounds)























































