Downloaded 34 times
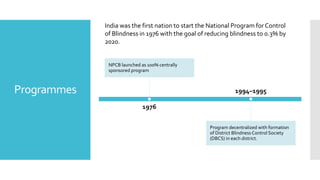











India launched the National Program for Control of Blindness (NPCB) in 1976 with a goal to reduce blindness from 1.4% to 0.3% by 2020. The program includes comprehensive eye care, community outreach, and partnerships to emphasize prevention and expand human resources. Recent initiatives focus on free presbyopia spectacles, mobile ophthalmic units, and raising awareness about eye donation.