This document discusses several conditions related to the male genitalia, including phimosis, paraphimosis, Peyronie's disease, and carcinoma penis.
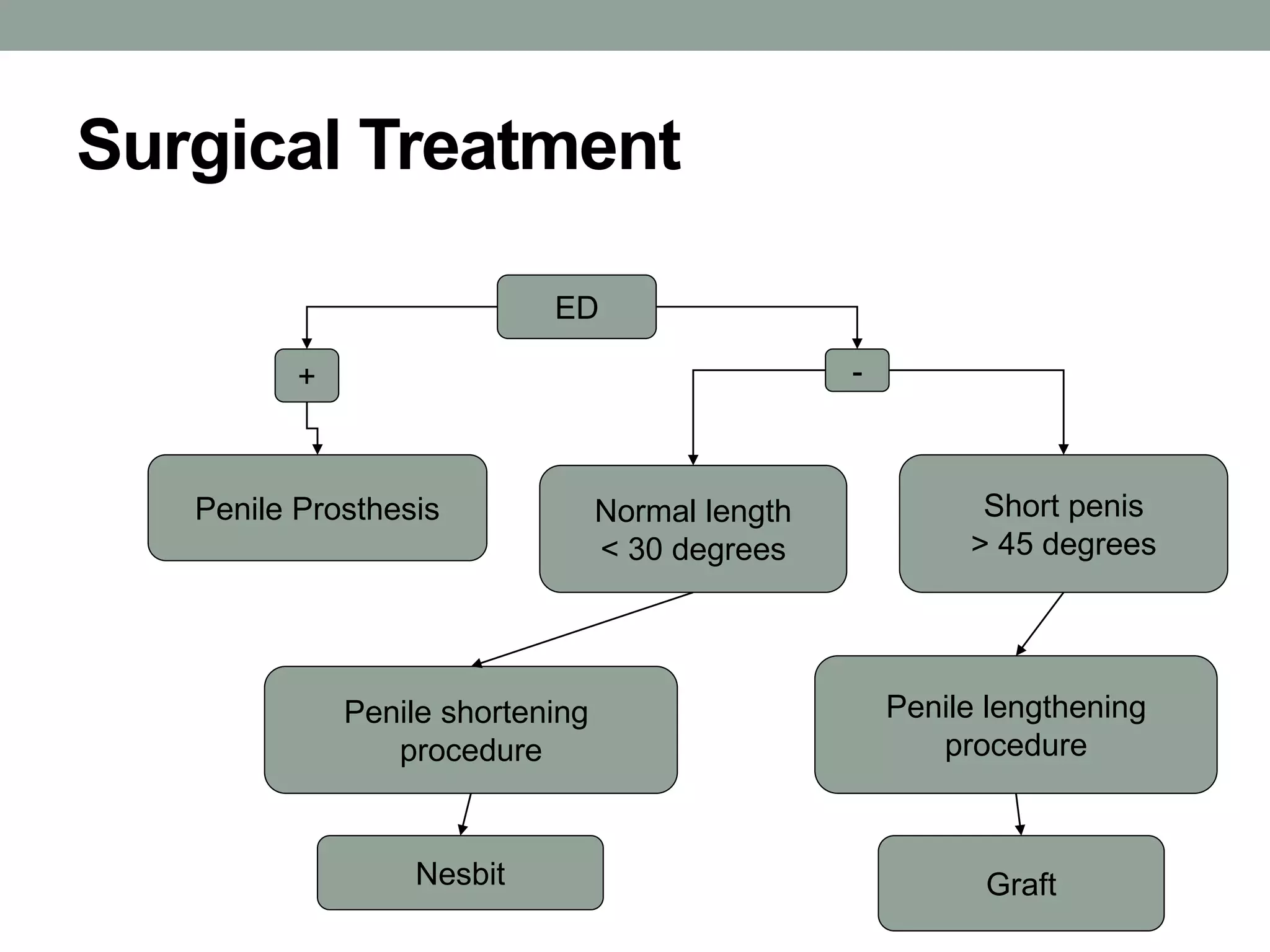
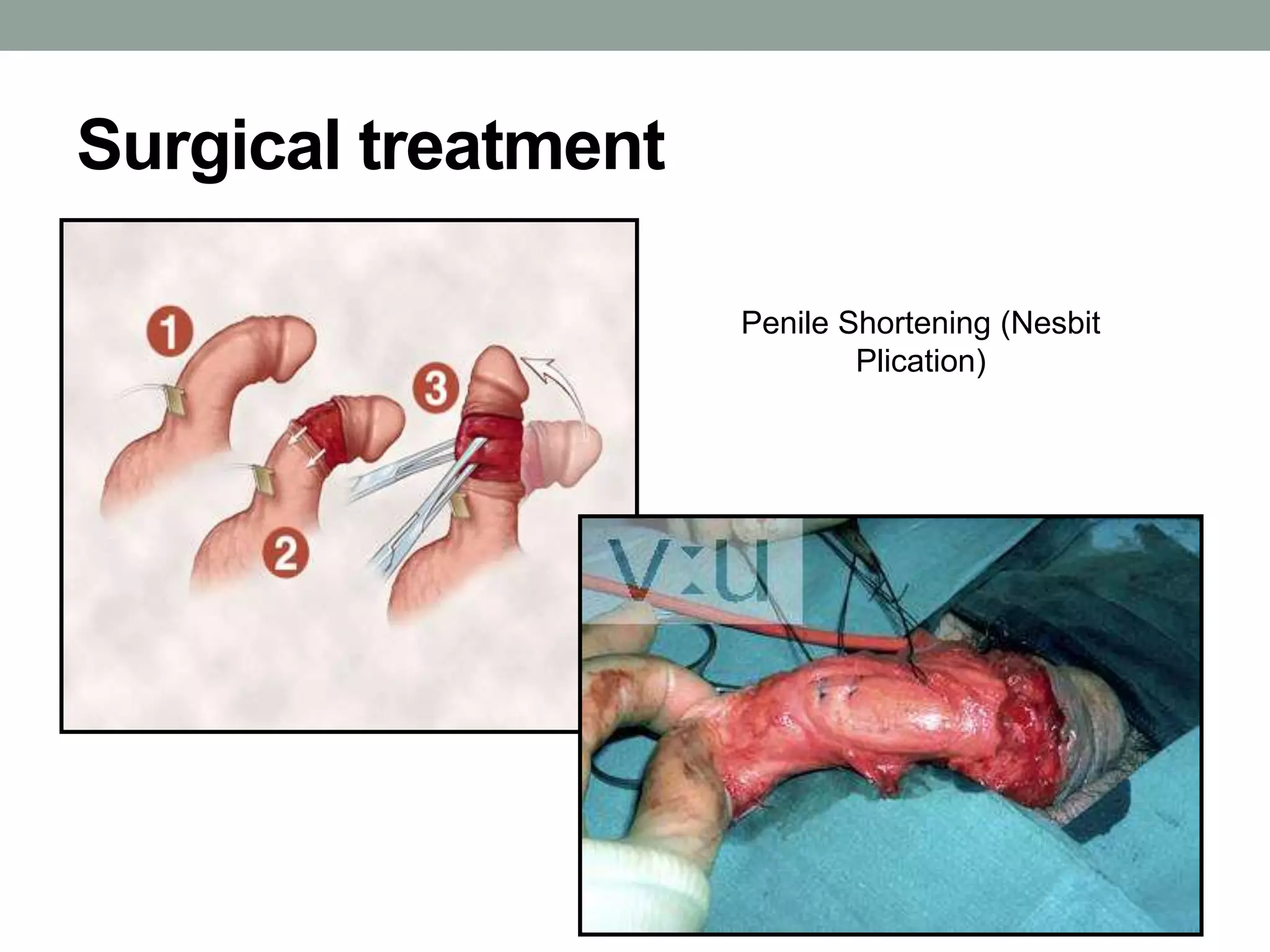
Phimosis is the inability to retract the foreskin over the glans penis. It can be physiologic in infants or pathologic due to scarring. Paraphimosis occurs when the trapped foreskin becomes edematous behind the glans. Peyronie's disease involves fibrosis and curvature of the penis during erection. Carcinoma penis is an uncommon cancer affecting the penis, which has higher rates in Africa and Asia. Risk factors include HPV infection and phimosis. Staging and treatment involve surgery and lymphadenectomy