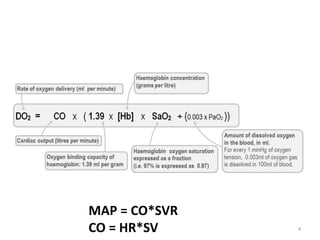
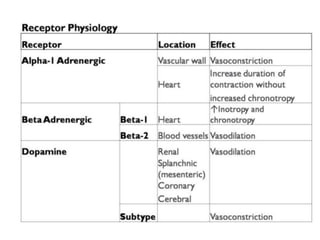
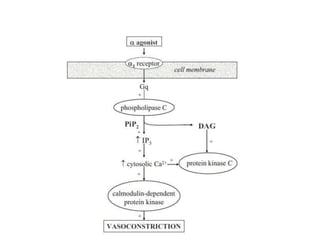
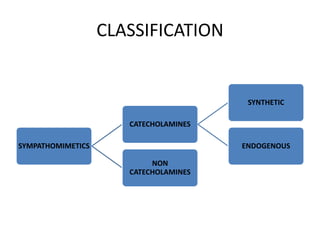
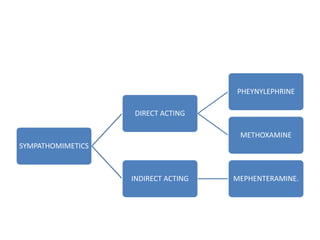
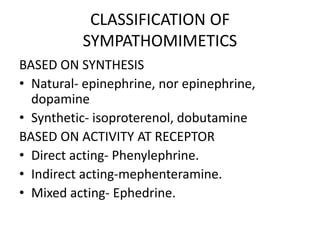
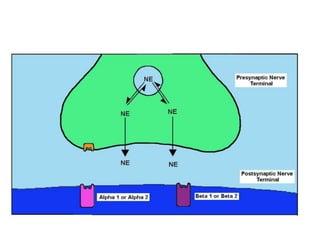
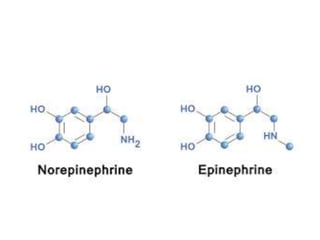
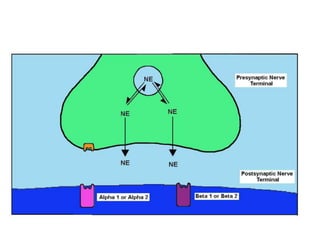
Vasopressors are drugs that induce vasoconstriction and elevate blood pressure. This document discusses the history, physiology, classification, and pharmacology of various vasopressors used in the ICU setting. It describes how vasopressors act on different adrenergic receptors to increase blood pressure by either increasing cardiac output, systemic vascular resistance, or both. The document reviews commonly used vasopressors like norepinephrine, epinephrine, dopamine, phenylephrine, dobutamine, and ephedrine - outlining their indications, mechanisms of action, pharmacokinetics, and adverse effects.