Download to read offline
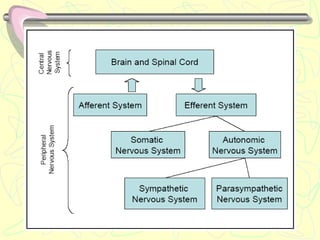
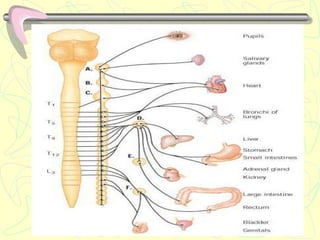
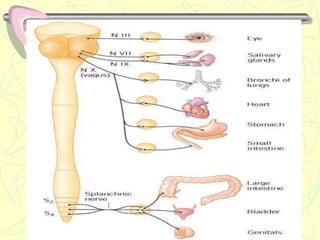
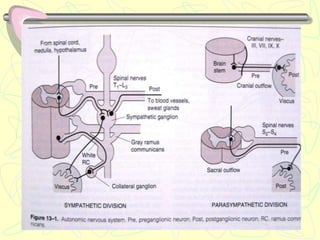
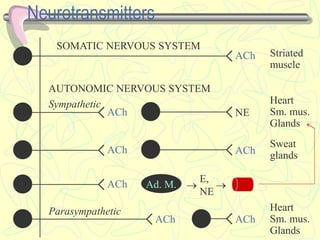
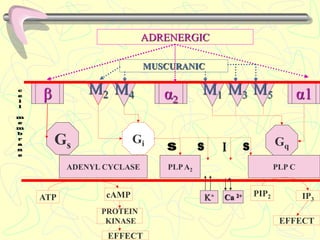
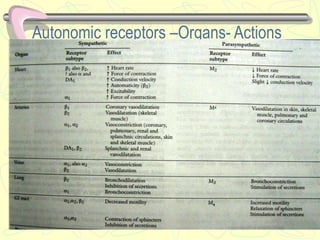
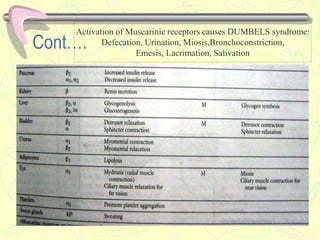
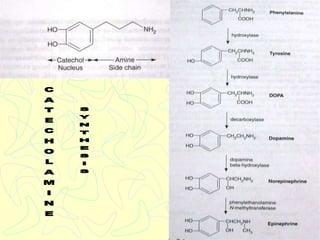
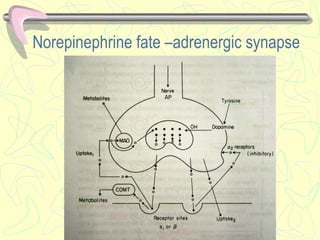
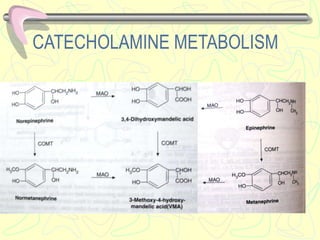
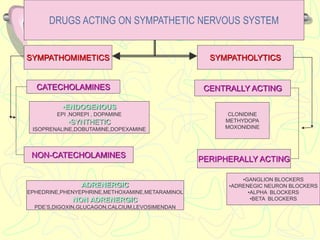
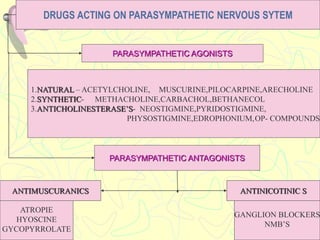

This document discusses drugs that act on the autonomic nervous system. It covers neurotransmitters in the somatic and autonomic nervous systems like acetylcholine and catecholamines. It then categorizes and describes drugs that act on the sympathetic and parasympathetic nervous systems, including sympathomimetics, sympathomolytics, parasympathomimetics, and parasympatholytics. Specific drugs are discussed in detail including their mechanisms, uses, doses, and side effects.















































