Downloaded 493 times
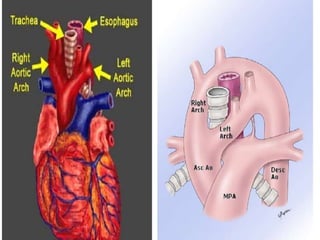
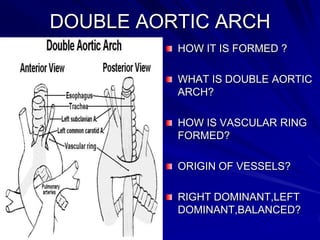
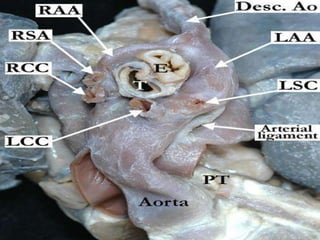
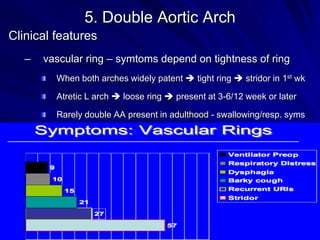
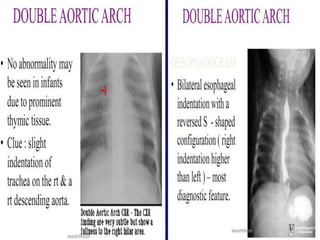
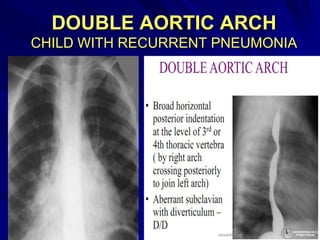

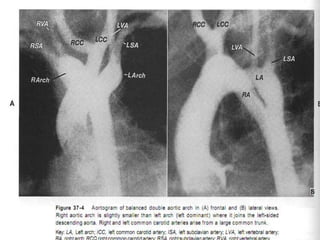
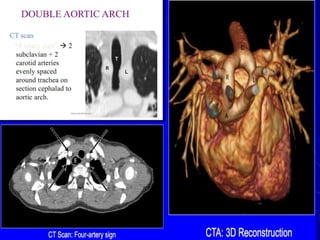
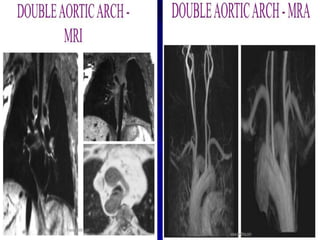
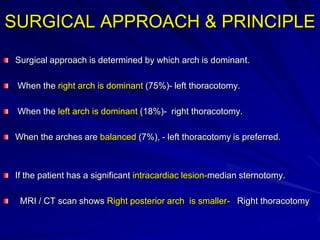
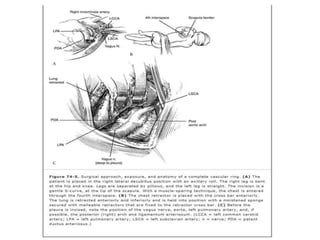
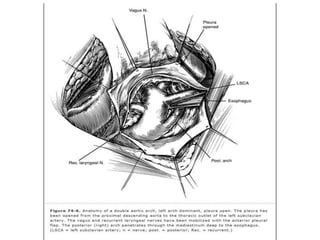
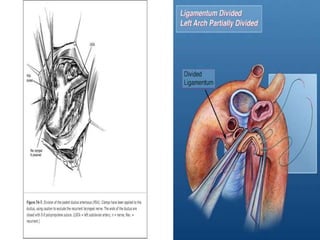
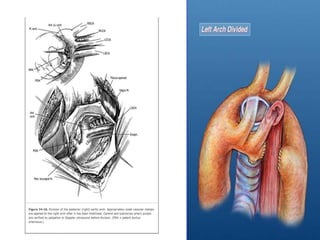
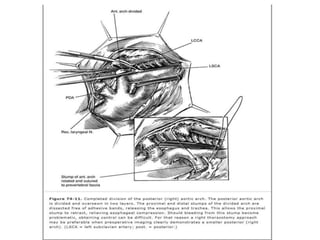
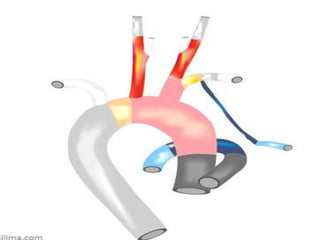
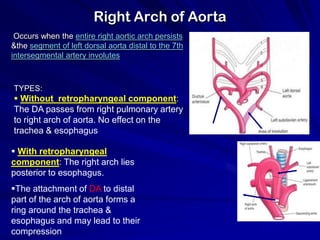
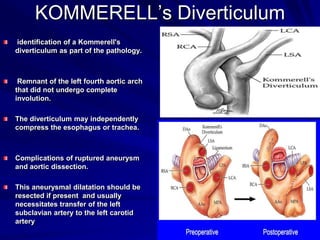

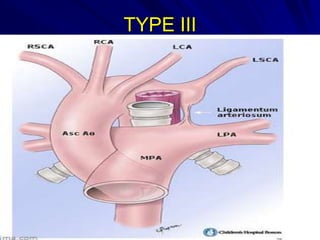
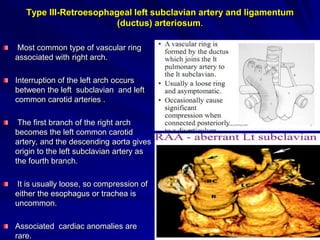
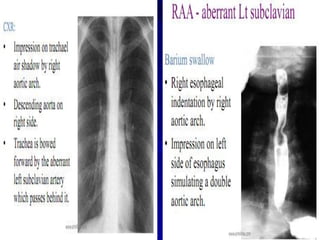
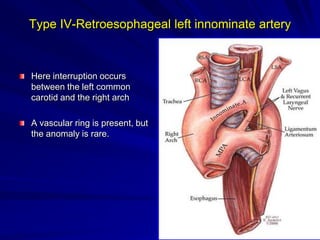
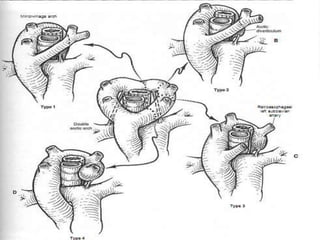
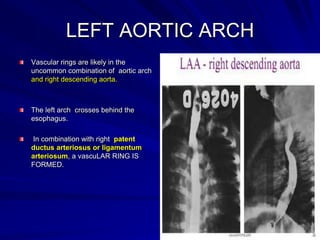
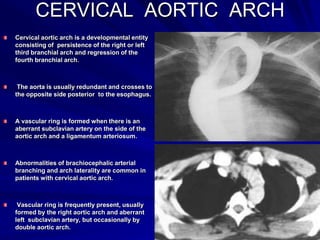
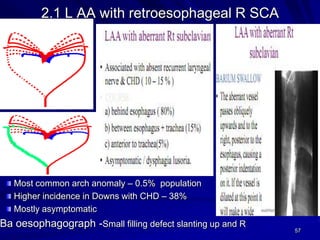
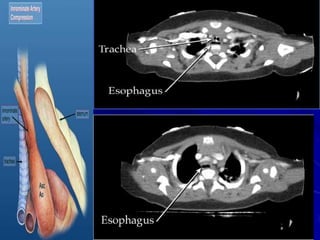


The document discusses various types of vascular rings and slings that can form due to abnormalities in aortic arch development, including double aortic arch where both right and left arches are present and form a ring around the trachea and esophagus, and right aortic arch with an aberrant retroesophageal ligamentum arteriosum. It provides details on the embryology, clinical presentations, investigations, and surgical techniques for repairing different types of vascular rings and slings.























































































