Uvea: Anatomy, Nerve & Vascular Supply, Clinical Correlation
•Download as PPTX, PDF•
55 likes•11,665 views

This document provides an overview of the anatomy, nerve and blood supply of the uvea, which includes the iris, ciliary body, and choroid. It begins with an introduction to the uvea and its embryological development. It then discusses the anatomy and structures of the iris, ciliary body, and choroid in detail. It also reviews the blood supply and some clinical applications related to the uvea. The document is presented as part of an optometry lecture covering this topic in detail over several slides.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Uvea: Anatomy, Nerve & Vascular Supply, Clinical Correlation
Similar to Uvea: Anatomy, Nerve & Vascular Supply, Clinical Correlation (20)
More from Sarmila Acharya
Recently uploaded
Recently uploaded (20)
Uvea: Anatomy, Nerve & Vascular Supply, Clinical Correlation
- 1. UVEA: ANATOMY, NERVE & VASCULAR SUPPLY, CLINICAL CORRELATION Presenters: Suraj Thapa Magar Sarmila Acharya 2nd year B.Optometry Resource person: Mr. Niraj Dev Joshi
- 2. Presentation Layout 1) Introduction 2) Embryology of the Uveal tract 3) Congenital anomalies of Uveal tract 4) Iris: anatomy and nervous supply 5) Ciliary body: anatomy and nervous supply 6) Choroid: anatomy 7) Blood supply of Uveal tract 8) Clinically applied aspects 9) References
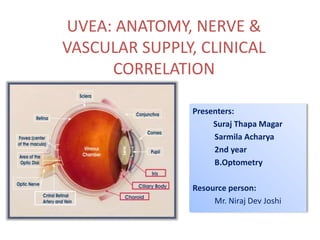
- 3. • Coined from latin word uva - grape • Middle vascular coat of eyeball • From anterior to posterior: - Iris - Ciliary body - Choroid INTRODUCTION
- 4. Uveal tract firmly attached to sclera only at 3 sites • The scleral spur • The exit points of vortex veins • The optic nerve
- 5. Embryology NEUROECTODERM Epithelial layers of the iris Sphincter and dilator pupillae muscles Epithelial layers of the ciliary body PERIOCULAR MESENCHYME Blood vessels of iris, choroid, ciliary body Stroma of iris Ciliary muscle and stroma of ciliary body Choroid
- 6. Milestones 9th week of gestation Ciliary body begins to appear 12th week of gestation Sphincter pupillae appears 4th month Ciliary processes fully formed 5th month Iris and choroid are formed 6th month Dilator muscles begin to form Sphincter muscle fully differentiated Postnatal period dilator muscles reach adult proportion by 5 years
- 7. Sometimes strands of this tissue are left as Persistent pupillary m/m Towards end of gestation , the central iris stroma (pupillary m/m) disappears forming pupil. -Represents remnants of vascular sheath of lens -Strands arise from and insert into iris collarette. The dilator muscle is not apparent until sixth month, and differentiation of myoepithelial cells continues after birth→pupillary miosis
- 8. Congenital Anomalies of Uveal Tract Aniridia Partial or complete absence of iris True aniridia : rare A peripheral rim of iris present (although hypoplastic) & this is called clinical aniridia
- 9. Heterochromia of iris Heterochromia Iridium Heterochromia Iridis Color of one iris differs from the other One sector of iris differs from the remainder of iris
- 10. Corectopia • Displacement of pupil • Bilateral and symmetric • A/w ectopia lentis, and the lens and pupil are commonly dislocated in opposite directions Polycoria • More than one opening in the iris • Result of local hypoplasia of iris stroma and pigment epithelium
- 11. Colobomas Colobomas represent an absence of tissue may occur anywhere along optic fissure and can affect the iris, choroid, macula & optic nerve Because optic fissure closes first at equator of eye, & then in a posterior and anterior direction, colobomas are most frequently found at the two ends of the optic fissure, i.e iris and optic nerve Generally Choroidal /Fetal Fissure Closes by 6th wk of gestation Failure to fuse results typical COLOBOMAS
- 12. Uveal coloboma - Coloboma : a condition where a portion of the structure is missing Typical coloboma: Located inferonasally in the region of closure of embryonic fissure a. Complete coloboma: Extends from pupil to optic nerve Includes retina, choroid, ciliary body, iris b. Incomplete coloboma: Involve the iris alone, or iris and ciliary body, or iris, ciliary body & part of choroid
- 13. Atypical coloboma - Occasionally found in other positions i.e. not related to fissure closure - It is usually incomplete
- 14. Greek Word iris - color haloes/rainbows Anterior most part of uvea Diameter -12 mm Thickness -0.5 to 0.6 mm 3 to 4 mm aperture slightly nasally- pupil Attached to middle of anterior surface of ciliary body Thinnest at root and tears easily away from its attachment to ciliary body : Iridodialysis IRIS
- 15. POINTs TO BE NOTED Pupillary margin rests lightly on anterior surface of lens so when lens is removed iris is flat and often tremulous: IRIDODONESIS CYCLODIALYSIS is separation of ciliary body from scleral spur, creating a direct connection betwn anterior chamber and suprachoroidal space increases aqueous outflow and predisposes the eye to hypotony
- 16. Macroscopic structure Anterior surface 1. ciliary zone: - radial steaks - crypts: peripheral & central - contraction furrows 2. Pupillary zone: between collarette and pigmented pupillary frill
- 18. Posterior surface - dark brown or black - looks smooth Under Magnification: -schwalbe’s contraction folds: radial furrows, commence 1mm from pupillary border -schwalbe’s structural furrows: start 1.5mm from pupillary border, narrow and deep to start with but becomes wide and shallow as they approach the ciliary margin -circular furrows: finer than radial furrows cross the structural furrows at regular interval more marked near the pupil
- 19. Contact between the posterior surface of iris and anterior capsule of the lens is also altered by pupillary size It is greatest on mid dilatation Precipitate angle closure glaucoma in some predisposed eye with narrow angle
- 20. Microscopic structure 1. Anterior limiting layer 2. Iris stroma 3. Anterior epithelial layer 4. Posterior pigmented epithelial layer
- 21. 1. Anterior limiting membrane • Condensed part of the stroma • Consists of melanocytes and fibroblasts • Deficient in areas of crypts, very thin at contraction furrows • Determines the color of iris 3 types of intercellular junctions present - Gap junctions - Intermediate junctions - Discontinuous tight junctions
- 22. 2. Stroma • Main bulk of iris tissue • Consists of loosely arranged collagenous network with mucopolysaccharide ground substance contains -The sphincter pupillae muscles - Dilator pupillae muscles -The vessels and nerves of iris -Cellular elements: fibroblast, melanocytes, clump cells and mast cells
- 23. Sphincter pupillae muscles - 0.7mm wide , 0.1-0.17mm thick - Encircles pupillary margin - lies in stroma deep to the surface - - Even after broad iridectomy , which removes a sector of iris sphincter,the remaining sphincter can still constrict the remaining pupil margin Origin is from anterior epithelium,but actually separated from this layer by a thin sheet of collagen & dilator fibre processes, to which it is firmly bound. -Innervated by parasympathetic via short ciliary nerve
- 24. Dilator pupillae muscle - 60um long &7um wide - Filled with myofilaments - Extend from iris root towards pupil - When the muscle contract,it pulls the pupillary margin towards the ciliary body, dilating the pupil - Innervated by sympathetics via long ciliary nerve
- 25. Parasympathetic Control of pupillary Size Sphincter Pupillae Short ciliary Nerve Ciliary Ganglion Inferior Oblique Muscle Oculomotor Nerve Edinger Westphal Nucleus
- 26. Dilator muscle Long ciliary nerve Ciliary ganglion Ophthalmic division of Vth nerve Cervical ganglion Ciliospinal centre of Budge Posterior Hypothalamus Sympathetic Control of Pupillary Size:
- 28. Blood vessels - Form bulk of iris stroma - They arise mainly from circulus arteriosis major - Some also arise directly from anterior ciliary arteries -Responsible for radial streaks seen on anterior surface of iris Peculiarities of Iris : Absence of internal elastic lamina non fenestrated capillary endothelium
- 29. Cellular elements of stroma 1) Fibroblast • Most common stromal cell • Found around blood vessels, nerves, muscle tissue and throughout the iris substance 2) Melanocytes • Branching elements with processes • Contain melanin granules
- 30. 3) Clump cells • large round pigment cells without processes • filled with inclusion granules 4) Mast cells • They are round • Have villous processes Extracellular matrix of stroma -Contain type VI collagen -Laminin and fibronectin
- 31. 3. Anterior Epithelial Layer • Anterior continuation of pigment epithelium of ciliary body • Lacking of melanocytes • Basal processes of the cells of this layer give rise to dilator pupillae muscle
- 32. 4. Posterior pigmented epithelial layer • Anterior continuation of non pigmented epithelium of ciliary body which in turn is the continuation of sensory retina • Contain abundant columnar type pigment cells • It curves around the pupillary margin and extends for a short distance onto anterior border layer of iris stroma as the pigment ruff.
- 33. - presence of iris pigment epithelium on anterior surface of iris - Congenital or a/w rubeosis irides, neurofibromatosis,etc Clinical significance Ectropion uveae
- 34. Forward bowing of iris Angle closure glaucoma Contact between the posterior surface of iris and lens creates a relative pupillary block to the flow of aqueous humor through the pupil,which is more marked in mid dilatation
- 35. Applied anatomy Iris Nodules - Accumulated deposits of epithelioid cells and lymphocytes deposited onto the iris without tissue destruction. Two types: Koeppes nodule at pupillary border Busaccas nodules near collarette
- 36. Iris Atrophy - Areas of degeneration of iris - Commonly seen in iridocyclitis
- 37. • Forward continuation of the choroid at ora serrata • In cut section, triangular in shape CILIARY BODY
- 38. • Anterior side of triangle- part of anterior chamber angle • In middle- attached to the iris • Outer side of triangle- lies against the sclera with a suprachoroidal space in between • Inner side of triangle divided into 2 parts: 1) Pars plicata-anterior 2) Pars plana-posterior
- 39. 1) Pars plicata / corona ciliaris • Anterior part • About 2 to 2.5 mm long • Contain ciliary muscles • Have finger like ciliary processes 2) Pars plana / orbicularis ciliaris • Posterior smooth part • 5mm wide temporally • 3 mm wide nasally
- 41. Microscopic structure From without inwards, consists of five layers: 1) Supraciliary lamina 2) Stroma of the ciliary body 3) Layer of pigmented epithelium 4) Layer of non-pigmented epithelium 5) Internal limiting membrane
- 42. 1) Supraciliary lamina • Outermost condensed part of stroma • Consists of pigmented collagen fibres • Continuation of suprachoroidal lamina • Anteriorly, continues with the anterior limiting membrane of iris 2) Stroma of the ciliary body • Consists of collagenous connective tissue and fibroblast • Embedded in it: a. Ciliary muscle b. Blood vessels c. Nerves d. Pigment cells & other cells
- 43. Ciliary muscle • Non striated muscle • Occupies most of the outer part of the ciliary body Three main groups: 1) The longitudinal or meridional fibres 2) The oblique or radial fibres 3) The circular fibres
- 44. 1) Longitudinal or meridional fibres -Most external and closest to the sclera -Pass posteriorly into the stroma of ciliary body 2) Oblique or radial fibres -Radiate out from the scleral spur 3) Circular fibres -Occupy anterior and inner portion of the ciliary body -Nearest to the lens -Runs parallel to the limbus -Directly act as sphincter
- 45. Main action of all parts of ciliary muscles is to slacken the suspensory ligament of lens & thus helps in Accommodation. -Longitudinal muscle fibres form tendinous attachment to the scleral spur: their contraction increases aqueous flow by opening up the spaces of trabecular meshwork
- 46. Contraction of the ciliary muscle,especially longitudinal and circular fibres pulls the ciliary body forward in accommodation.
- 47. Vascular stroma -Contains major arterial circle just in front of circular fibres - Arterial circle is formed by the anastomosis between the long posterior ciliary arteries and anterior ciliary arteries and send branches to iris and ciliary body
- 48. 3) Layer of pigmented epithelium • Forward continuation of RPE • Anteriorly, continuous with anterior epithelium of iris 4) Layer of non-pigmented epithelium • Consists mainly of low columnar or cuboidal cells • Forward continuation of sensory retina which stops at ora serrata. • Continues anteriorly with posterior pigmented epithelium of the iris
- 49. 5) Internal limiting membrane • Lines the non-pigmented epithelium • Forward continuation of internal limiting membrane of the retina.
- 50. Nerve supply of the ciliary body • Sensory fibres run from the nasociliary branch of the ophthalmic division of the trigeminal nerve, as the long ciliary nerve • These fibres enter the ciliary body and terminate in iris, cornea and ciliary muscle Sensory Nerves
- 51. Edinger Westphal nucleus Autonomic Nerves Parasympathetic fibres Oculomotor nerve Accessory Ganglion Short ciliary nerve Ciliary muscle
- 52. Ciliary processes • Whitish finger-like projections from pars plicata part of the ciliary body • 70 to 80 in number • Each process is about 2mm long and 0.5mm in diameter • Are the site of aqueous production
- 53. Ultrastructure of ciliary processes Consists of: a. The network of capillaries b. Stroma of ciliary processes c. Two layers of epithelium
- 54. a. The network of capillaries • Occupies the centre of each process • Each capillary consists of a very thin endothelium with fenestration • Lined by basement m/m • Mural cells or pericytes present within basement membrane
- 55. b) Stroma of the ciliary process • Very thin • Separates capillary network from epithelial layers • Consists of ground substance: mucopolysaccharide, proteins & solute of plasma • Few collagen connective tissue fibres • Wandering macrophages
- 56. c) Two layers of epithelium • Their apical surfaces in apposition to each other Outer pigmented epithelium: • Contains numerous melanin granules Inner non-pigmented epithelium: • Contain mitochondria, zonula occludentes & lateral and surface interdigitations • The tight junction between cells of this layer form blood aqueous barrier
- 58. • Posterior portion of the middle vascular coat • Extremely vascular • Extends from optic disc to ora serrata • The inner surface: smooth, brown and lies in contact with RPE • The outer surface: rough and attached to sclera • Posteriorly-0.22 mm thick • Anteriorly-0.1 mm CHOROID
- 59. • Firmly attached to the margin of the optic disc • Loosely at points where vessels and nerves enter it • Attachment to sclera is strongest
- 60. Microscopic Structure From without inwards, consists of four layers: 1) Suprachoroidal lamina (lamina fusca) 2) Stroma of the choroid 3) Choriocapillaries 4) Bruch’s membrane (basal lamina or lamina vitrae)
- 61. 1) Suprachoroidal lamina • Thin membrane 10 to 34 μm • Made of condensed collagen fibres, melanocytes and fibroblasts • Continues anteriorly with supraciliary lamina • Space between this m/m and sclera: suprachoroidal space (contain long & short posterior ciliary arteries and nerves)
- 62. -Contains vessels, nerves, cells & connective tissue -Stromal cells include: a. Melanocytes b. Fibrocytes c. Macrophages d. Mast cells e. Plasma cells 2) Stroma of the choroid Main bulk is formed by vessels, arranged in two layers: a. Haller’s layer: outer layer of large vessels b. Sattler’s layer: inner layer of medium vessels
- 63. • Consists of a rich bed of wide bore fenestrated capillaries (18 to 50μm) • Receives most of its blood from medium & large vessels of stroma • Nourishes RPE & outer layers of sensory retina • Density greatest at macula 3) Choriocapillaries • Choriocapillaries are divided into non overlapping lobules or hexagonal patches
- 64. • Innermost layer of choroid • Thin non cellular lamina • Lies between choriocapillaries and pigment epithelium of the retina • 2 to 4 μm thickness 4) Bruch’s membrane
- 65. Comprises of five layers a. Basal lamina of RPE b. Inner collagen layer c. Middle elastic layer d. Outer collagen layer e. Basal lamina of choriocapillaries
- 66. • Choroidal ischaemia often occurs as a pale hexagonal patches (mosaic pattern) • During choroidal phase of FFA, these lobules fill independently from one another, giving a transiently patched or blotched appearance Clinical significance
- 67. Bruch’s membrane become thickened with increasing age and produces hyaline excrescence known as Drusens
- 68. Uveal tract supplied by 3 sets of arteries: 1) Short posterior ciliary arteries 2) Long posterior ciliary arteries 3) Anterior ciliary arteries BLOOD SUPPLY OF THE UVEAL TRACT
- 70. 1) Short posterior ciliary arteries Arise as two trunks from the ophthalmic artery Each trunk divides into 10 to 20 branches Pierce the sclera around the optic nerve Supply the choroid in segmental manner
- 71. 2) Long posterior ciliary arteries Arise as nasal and temporal branch from the ophthalmic artery Pierce the sclera obliquely on medial & lateral side of optic nerve Run forward in suprachoroidal space to reach ciliary muscle, without giving any branch Anastomose with each other & with the anterior ciliary arteries to form major arterial circle And give branches which supply the ciliary body
- 72. 3) Anterior ciliary arteries Derived from muscular branch of ophthalmic artery 7 in number: 2 each from arteries of SR, IR & MR, 1 from that of LR Pass anteriorly in the episclera Give branches to sclera, limbus & conjunctiva Ultimately pierce the sclera near the limbus to enter ciliary muscle
- 73. Anastomose with two long posterior ciliary arteries to form major arterial circle Several Branches arise from major arterial circle & supply ciliary process (one branch for each process) Many branches from major arterial circle run radially through iris towards pupillary margin Anastomose with each other to form minor arterial circle
- 75. • Four in number (superior temporal, inferior temporal, superior nasal and inferior nasal) • Pierce sclera obliquely on each side of SR and IR muscles about 6 mm behind the equator Venous Drainage Venae vorticosae (vortex veins or posterior ciliary veins)
- 76. • Two superior vortex veins open into superior ophthalmic vein • Two inferior vortex veins open into inferior ophthalmic vein
- 77. Uveitis: Inflammation of Uveal tissue only Classification: 1.Anterior uveitis: Some Clinically Applied Aspects Inflammation of Uveal tissue from iris upto pars plicata of ciliary body -Iritis: inflammation predominantly affect iris -Iridocyclitis: iris and pars plicata part of ciliary body are involved -Anterior cyclitis: pars plicata part of ciliary body is predominantly affected
- 78. 2.Intermediate Uveitis: Inflammation of pars plana and peripheral part of retina and underlying choroid 3.Posterior Uveitis: Inflammation of choroid and retina Hence the term choroiditis, chorioretinitis, retinochoroiditis or neurouveitis is used 4.Panuveitis: Inflammation of whole uvea
- 80. Pain Redness Photophobia Salient features of Uveitis
- 81. Posterior synechiae Cataract Glaucoma due to PAS Band keratopathy Posterior synechiae Cataract Glaucoma due to PAS Band keratopathy Complications of uveitis
- 82. Common clinical signs a) Aqueous Cells: -Presence of inflammatory cells in the anterior chamber -The inflammatory response causes white blood cells such as neutrophils, monocytes and lymphocytes to leave the inflamed iris vessels to reach aqueous humour.
- 83. Aqueous Flare: - Turbidity of the aqueous humour caused by increased protein level - Blood aqueous barrier breakdown results in protein (albumin) exudation in the anterior chamber giving the normally clear, colorless aqueous humour a milky appearance k/a flare
Editor's Notes
- Anterior balloons figure
- Development of iris is a/w formation of anterior portion of tunica vasculosa lentis. The developing vessels extend into mesenchymal cells that cover anterior lens surface and will ultimately be incorporated into iris stroma The most anterior region of tunica vasculosa lentis is replaced subsequently by pupillary m/m Anterior epicapsular remnants of tunica vasculosa lentis gives Persistent pupillay membrane
- Polycoria is a condition in which there are many openings in the iris that result from local hypoplasia of the iris stroma and pigment epithelium. True polycoria actually is a condition in which there is more than one pupil and the multiple pupils all have a sphincter and the ability to contract
- Iridodialysis, / coredialysis,.
- Cyclodylysis :typically occur in the setting of trauma or intraocular surgery. They have been reported following trabeculectomy, trabeculotomy, goniotomy, extracapsular cataract extraction, phacoemulsification, secondary intraocular lens (IOL) placement, phakic IOL removal, and displacement of an anterior-chamber IOL Iridodonesisis the vibration or agitated motion of the iris with eye movement.[1] This may be caused by lens subluxation,[2] the incomplete or partial dislocation of the lens; or by aphakia, the absence of a lens
- photograph
- Preganglionic fibre for both ciliary muscle n pupi arises from EWN which move along oculomoter nerve. At the anterior part of cavernous sinus the fibre moves along IO muscle n synapse at ciliary ganglion.From here 6-8 post ganglionic short ciliary nerve arises which then supplies to sphincter pupillae.
- 1st order neuron starts from posterior hypothalamus which runs through pons n medulla n finally synapse at C8-T2. 2nd order preganglionic axon travel along ventral root of c8-T2 n synapse at superior cervical ganglion at carotid bifurcation.3rd order neuron send their post ganglionic fibre through oph div of V nerve which enter into ciliary ganglion n reach dilator muscle as long ciliary nerve.
- Sphincter muscle encircles d pupil n innervated by parasym nerve endings n its contraction constrict d pupil.The dilator muscle runs radially n innervation is chiefly by sympathetic n contraction dilates d pupil
- Blood vessels of iris fig of wolff anatomy
- Neovascularisation of iris
- More marked in mid dilatation.This may encourage forward bowing of iris which in predisposed narrow angle may precipitate angle closure glaucoma
- Lisch nodules in neuofiromatosis
- Condn in which area of iris is degenerated
- The ciliary muscle behave like other smooth,non striated muscle fibres. Clinically the 3 groups of muscle fibres function as a unit ….presbyopia is a/w age-related changes in the lens rather than to changes in the ciliary muscle…even so,the muscle does change with age,with increasing amounts of connective tissue between the muscle bundles & a loss of elastic recoil after contraction
- Most of the ciliary muscle is made up of an outer layer of longitudinal fibres that attach to the scleral spur…. The radial muscle fibres arise in the midportion of the ciliary body …
- So the Cholinergic drugs contracts the ciliary muscle
- Ophthalmic nerve,smalllest of the three divisions of trigeminal nerve(5th nerve) has three branches…lacrimal,frontal & Nasociliary nerve. One of the branch of Nasociary nerve is The long ciliary nerves ,two in number,pierce the sclera on either side of optic nerve ,run forward between sclera & choroid and supply sensory nerves to the ciliary body, iris &cornea.
- Edinger –westphal nucleus,located in mid brain ,sends preganglionic fibers through the third cranial nerve i.e. oculomotor nerve to ciliary ganglion and accessory ganglion.Postganlionic nerve fibers from ciliary ganlion travel along the shrt ciliary nerve to supply the sphinter puppilae muscle and postganlionic fibers from the accessory ganlion supply the ciliary muscle. Parasympathetic activation of the M3 muscarinic receptors causes ciliary muscle contraction Sympathetic fibres have also been observed & may play a role in relaxing the muscle. Cervical sympathetic trunk-Synapse in superior cervical ganglion-Long ciliary nerve-Ciliary muscles
- 2 layer of epi r arranged wid apical surface in apposition to each other
- The tight junction between cells of Non- pigmented layer form blood aqueous barrier
- Patchy filling in ffa figure 3 phases Choroidal phase-8 to 12 sec after dye injection Arterial phase Venous phase Late phase
- (Drusens –tiny yellow or white accumulation of extracellular material that build up between Bruch’s membrane and RPE of eye) Drusen are yellow deposits under the retina. Drusen are made up of lipids, a fatty protein. Drusen likely do not cause age-related macular degeneration (AMD). But having drusen increases a person's risk of developing AMD. Exudate: a fluid with a high content of protein and cellular debris that has escaped from blood vessels and has been deposited in tissues or on tissue surfaces, usually as a result of inflammation
- They… …which…and.
- These are two in number &….these pierce..&…At the anterior end of ciliary muscle these anastomose
- Theese are derived from….these are 7 in number i.e,2 each from …..these arteries pass anteriorly….
- Where they anastomose with… to form Major arterial circle (circulus arteriosus major),near the root of iris…. …. Similarly many branches from this major arterial circle…….where they anastomose with each other to form Minor arterial circle (circulus arteriosus minor)
- A series of small veins which drain blood from the iris , ciliary body & choroid join to form the vortex vein. The vertex vein are four in number….they pierce the sclera…… behind the equator and drain into superior and inferior ophthalmic vein,which in turn drain into the cavernous sinus. Some drainage also occurs through the intrascleral venous plexus & the episcleral veins into the limbal region.
- But clinically there is always some associated inflammation of adjacent structures such as retina, vitreous,sclera n cornea
- from iris upto pars plicata of ciliary body pars plana and peripheral part of retina and underlying choroid Inflammation of choroid and retina
- Other features includes lacrimation and defective vision. Pain –ciliary spasm since ciliary body is innervated by trigeimina nerve.Redness due to dilated episcleral vessels.photophobia coz of inflammation of iris and cornea results irritation of corneal nerve n 2dary to ciliary spasm.
- Iris adheres to anterior crystalline lens during anterior uveitis.These are formed due to organisation of the fibrin rich exudate.Cycloplegics should be used to prevent posterior synechiae. atropine does not break the posterior synechia. Complicated cataracr may develop as a complication of persistent iridocyclitis. Secondary glaucoma due to ring synachie formation,not allowing the aqueous to flow from posterior to anterior chamber. BSK occurs as a complication of long-standing chronic uveitis .BSK is essentially a degenerative change a/w deposition of calcium salts in Bowman’s membrane, superficial stroma and deeper epithelium of cornea. transverse zone of opacification in the region of the palpebral fissure. The limbus region will remain clear.
- Now we r at the end of this pptn. Common clinical signs of ueitis are circumcorneal congestion,keratic precipitates,flare and cells,hypopyon etc. +1: 1-5cells, +2: 6-15cells, +3: 26-50cells, +4: over 50
- Given by SUN(standardization of Uveitis Nomenclature) +1:faint(just detectable) +2:moderate flare with clear iris and lens +3: marked flare(iris and lens details hazy) +4: intense flare(Fibrin or plastic aqueous
- Reiter syndrome-Triad of : Nonspecific urthritis Polyarthritis Conjunctival inflammation accompanied by iritis. Sympathetic Ophthalmia: Specific bilateral inflammation of the uveal tract due to chronic irritation of one eye, caused by a perforating wound to the eye or intraocular surgery, produces transferred uveitis in the fellow eye.