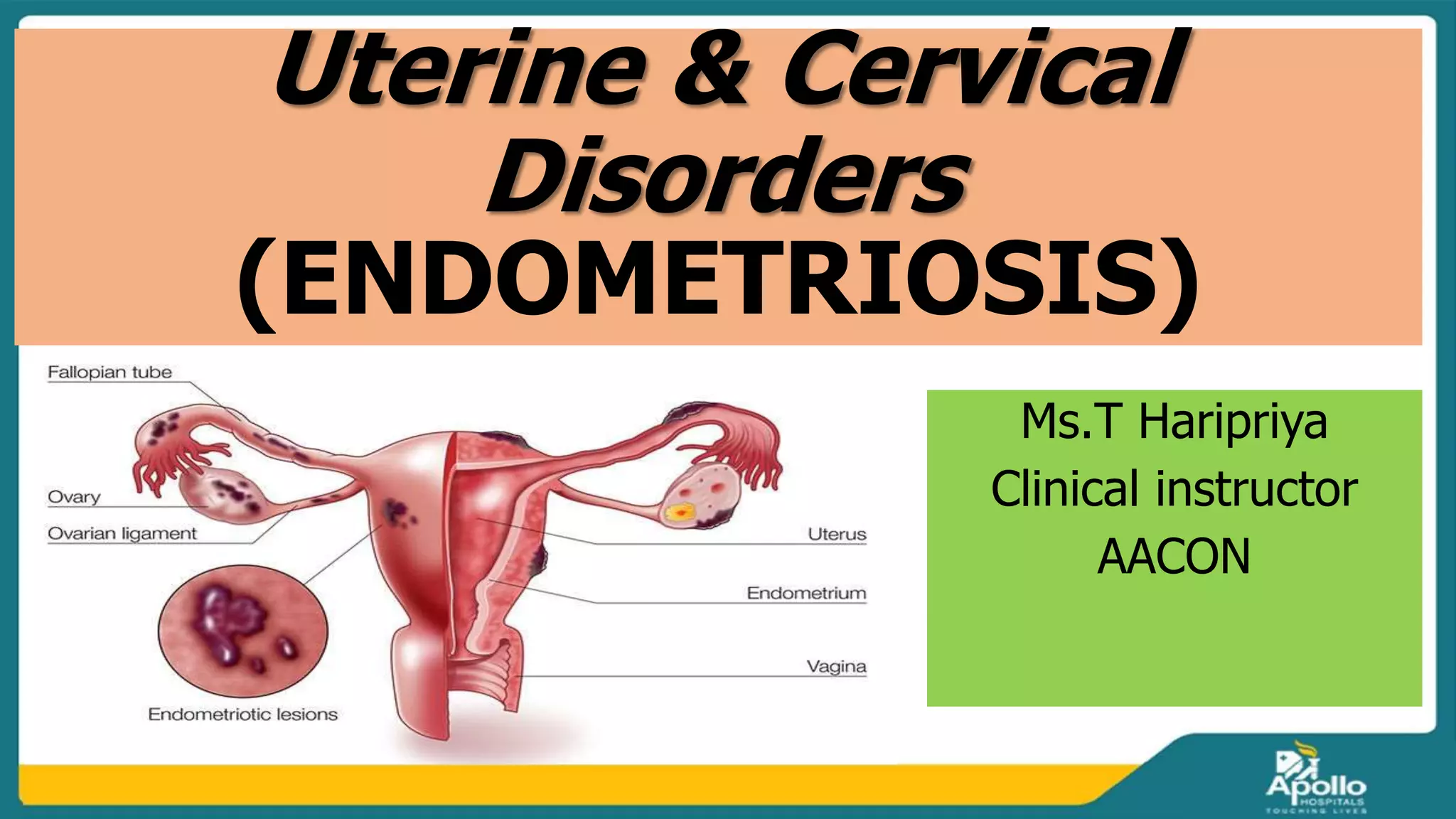
This document provides information on endometriosis, uterine polyps, and cervical polyps. It defines endometriosis as tissue similar to the endometrium growing outside the uterus, most often in the ovaries or surrounding tissues. Symptoms include irregular periods and infertility. Diagnosis involves laparoscopy or ultrasound and treatment includes hormonal therapy, NSAIDs, and surgery. Uterine and cervical polyps are non-cancerous growths that can cause irregular bleeding and are diagnosed by ultrasound, hysteroscopy, or biopsy before being removed by polypectomy or hysterectomy.