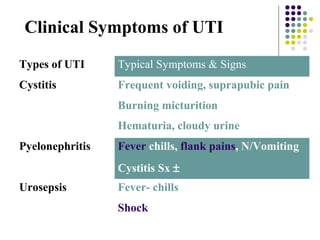
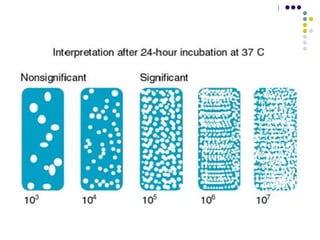
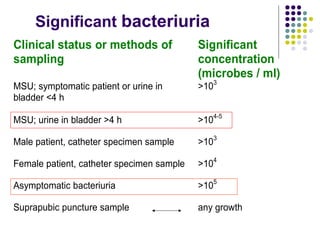
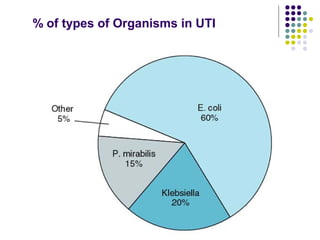
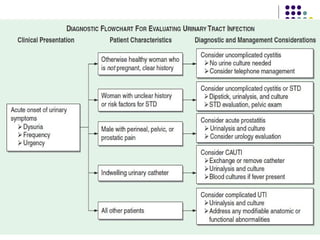
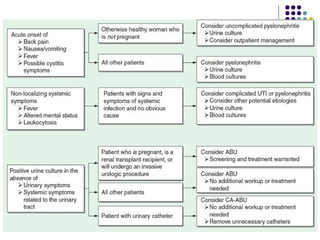
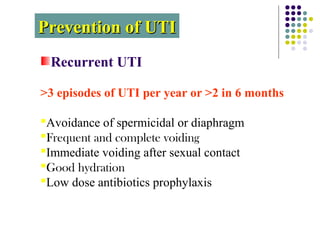
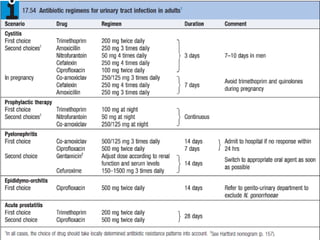

Urinary tract infections (UTIs) are very common, affecting around 150 million people worldwide each year. The majority are cystitis, with a smaller percentage being pyelonephritis. Risk factors include being female, as well as factors like urinary catheters and anatomical abnormalities. Escherichia coli is the most frequent cause of community-acquired UTIs. Diagnosis involves urinalysis, urine culture and sensitivity testing. Treatment consists of antibiotics targeting the identified organism. Recurrent UTIs may be prevented with low dose antibiotic prophylaxis.




































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


















