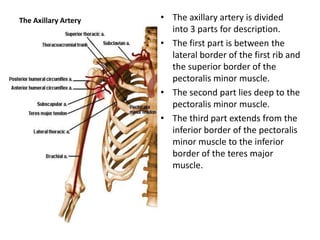
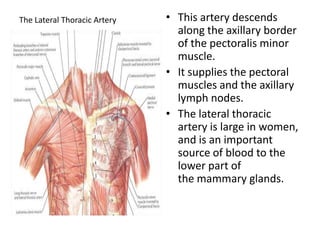
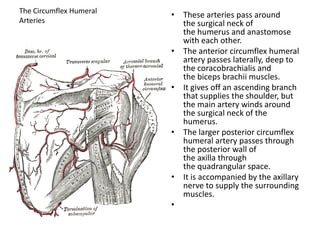
The document summarizes the major arteries of the upper limbs, including the axillary artery and its branches (thoracoacromial, lateral thoracic, circumflex humeral arteries), brachial artery and its branches (profunda brachii, ulnar collateral arteries), and the terminal branches - radial and ulnar arteries. It describes the course and branches of each artery as they supply structures in the arm, forearm, and hand.