Download to read offline

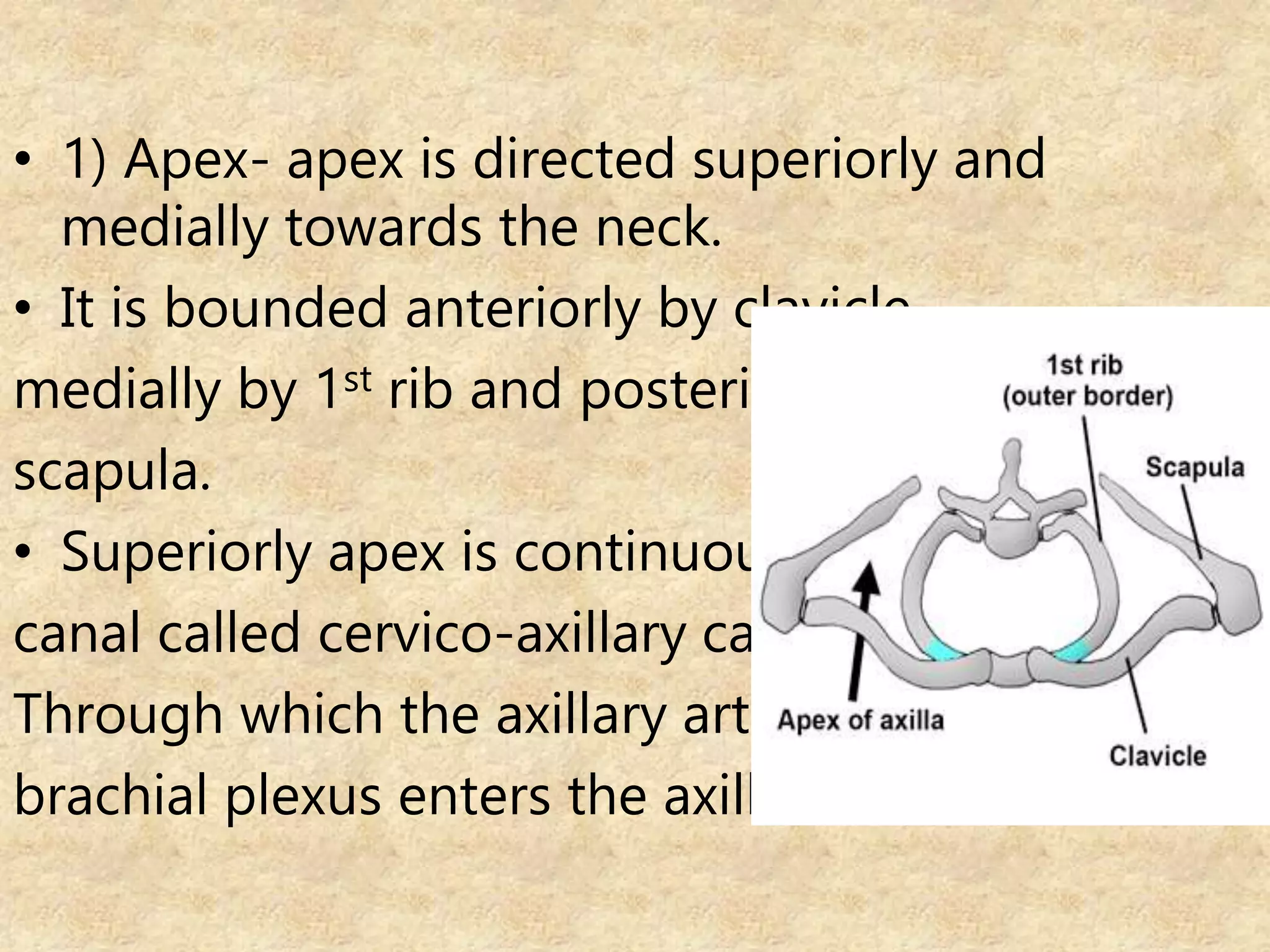








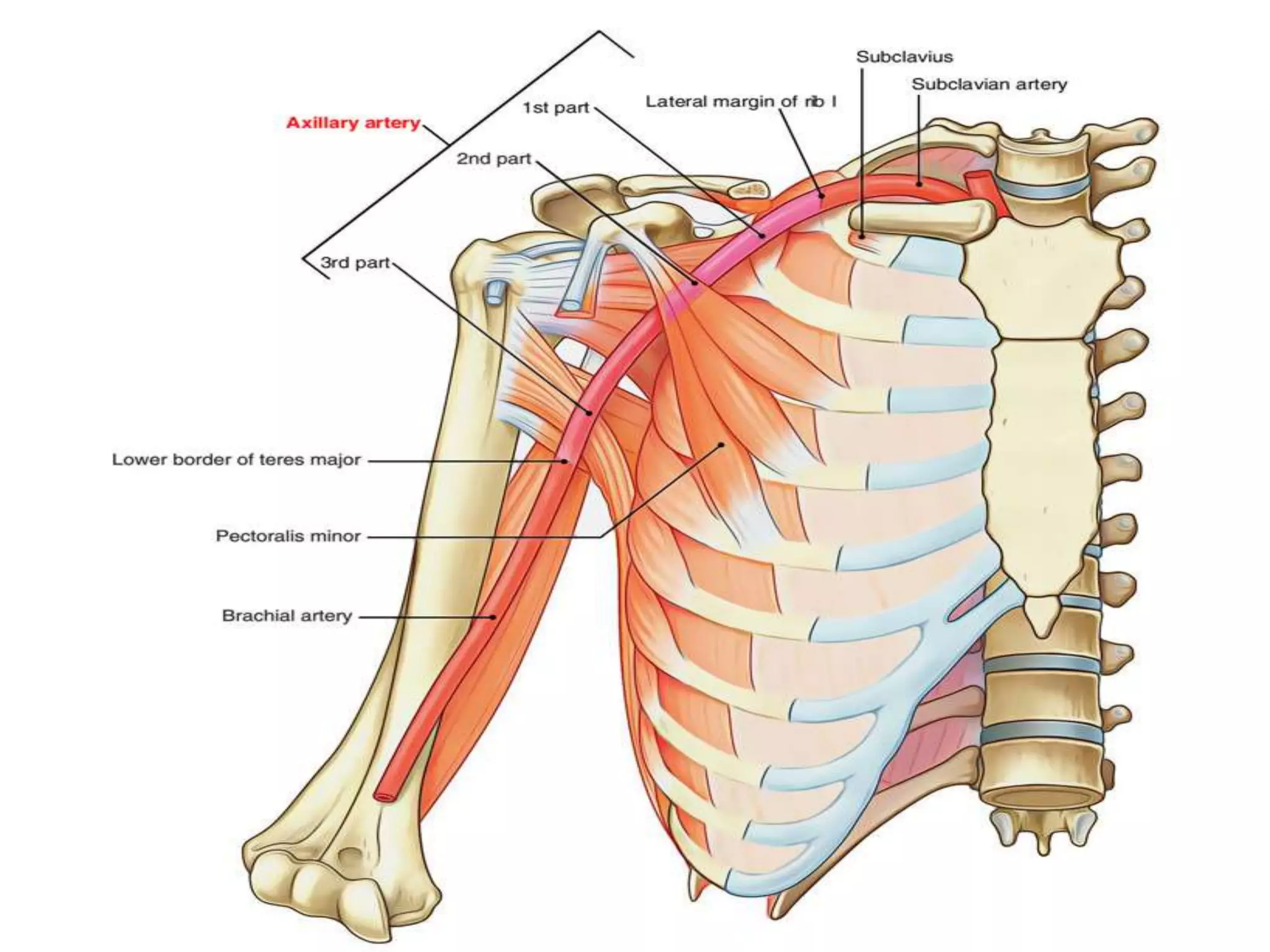














The document describes the anatomy of the axilla, subclavian artery, axillary artery, brachial artery, radial artery, ulnar artery, and intermuscular spaces in the arm. Key points include: - The axilla is a pyramidal space between the upper arm and chest wall containing lymph nodes, blood vessels and nerves. - The subclavian artery becomes the axillary artery in the axilla and then the brachial artery in the arm, with named branches along its course. - The radial and ulnar arteries are terminal branches of the brachial artery, running in the forearm and hand. - There are three intermuscular spaces in the arm that contain named


































![Lecture 25 Intermuscular sapces and axilla [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/lecture25intermuscularsapcesandaxillaautosaved-251110002658-47b36c78-thumbnail.jpg?width=640&height=640&fit=bounds)






































