Downloaded 388 times

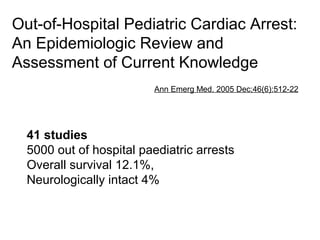
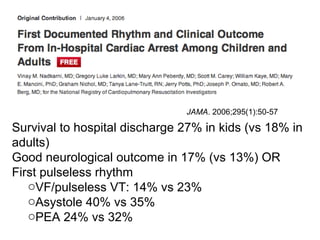
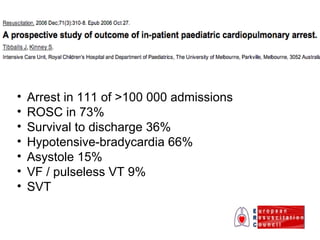




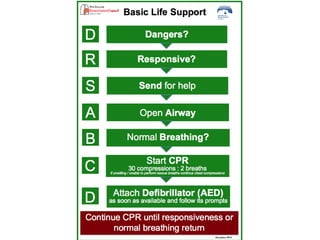
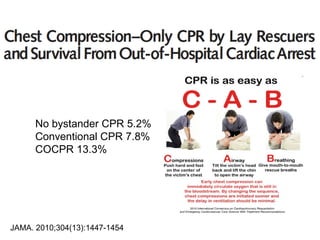

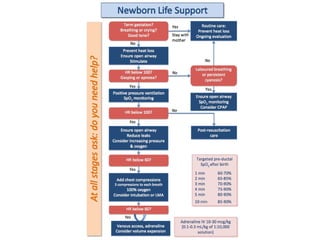
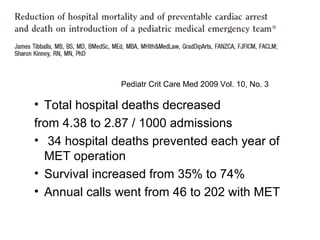

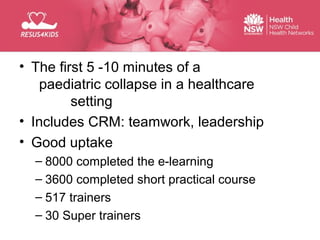
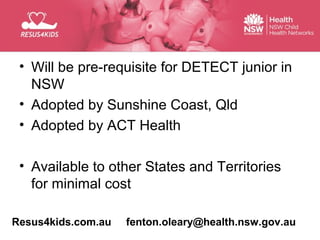

The document discusses updates in paediatric resuscitation, focusing on the scope of cardiac arrests in children both in and out of hospital settings. It highlights survival rates from various studies, the importance of training for medical teams, and improvements in paediatric emergency protocols. Additionally, it covers other relevant issues, such as family presence during resuscitation and the evolving approach to trauma management.