Downloaded 330 times






1. The document discusses perioperative nursing care, describing the three phases - preoperative, intraoperative, and postoperative. 2. In the preoperative phase, nurses conduct assessments, educate patients, and prepare them physically and psychologically for surgery. 3. The intraoperative phase involves monitoring the patient's physiological status and ensuring a sterile environment during the surgical procedure. 4. Different types of anesthesia are described, including general, local/regional, conscious sedation and spinal anesthesia, along with their risks and complications.



























































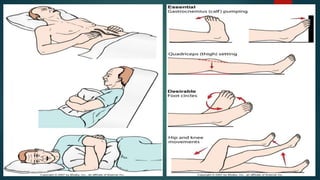
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


















![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)