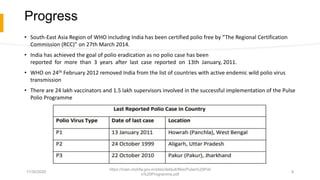
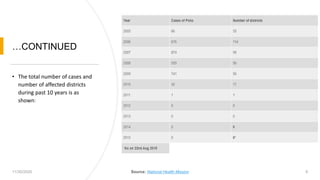
The document outlines the Pulse Polio Program in India, which was initiated in 1995 to achieve 100% coverage of the oral polio vaccine for children aged 0-5 years. Key achievements include India being declared polio-free by WHO in 2012, following no new cases since 2011, while it also discusses ongoing challenges such as surveillance lapses and risks from neighboring countries. Additionally, it emphasizes the importance of micro planning and community involvement to ensure effective immunization and respond to potential outbreaks.