Downloaded 466 times
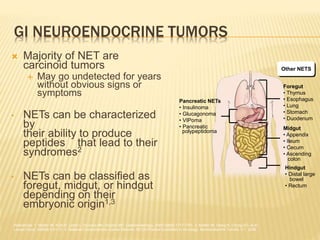
![NETS ARE THE SECOND MOST PREVALENT
TYPE OF GI MALIGNANCY
2x more prevalent
than pancreatic cancer
]
1. National Cancer Institute. SEER Cancer Statistics Review, 1975-2004. http://seer.cancer.gov/csr/1975_2004. 2. Modlin IM, Lye KD, Kidd M. Cancer. 2003;97(4):934-959.
]](https://image.slidesharecdn.com/neuroendocrinetumors1110-101123084847-phpapp02/85/Understanding-GEP-NET-Cancer-7-320.jpg)
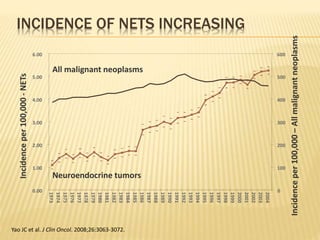
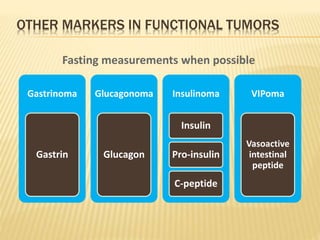
![Vague abdominal
symptoms
Primary tumor
Flushing
Metastases
Diarrhea
Death
NETS ARE OFTEN DIAGNOSED LATE
Time
Vinik A, Moattari AR. Dig Dis Sci. 1989;34[Suppl]:14S-27S.](https://image.slidesharecdn.com/neuroendocrinetumors1110-101123084847-phpapp02/85/Understanding-GEP-NET-Cancer-11-320.jpg)
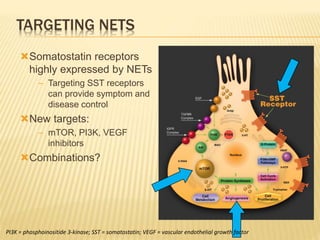

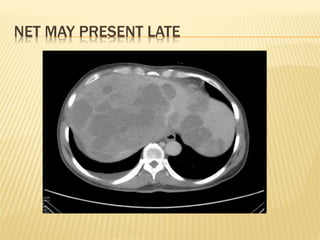
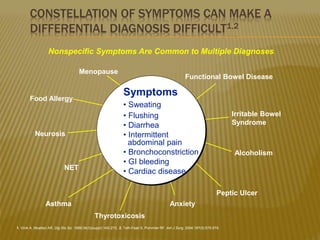
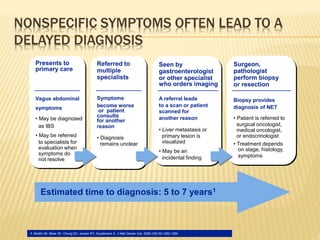
Neuroendocrine tumors (NETs) originate from neuroendocrine cells and are characterized by their ability to produce peptides linked to various syndromes. These tumors comprise a diverse group, including gastroenteropancreatic NETs and carcinoid tumors, which often present with vague symptoms leading to delayed diagnosis. Diagnosis typically involves clinical assessment, imaging, and specific tumor markers, with treatment options ranging from surgery to targeted therapies.