Downloaded 47 times






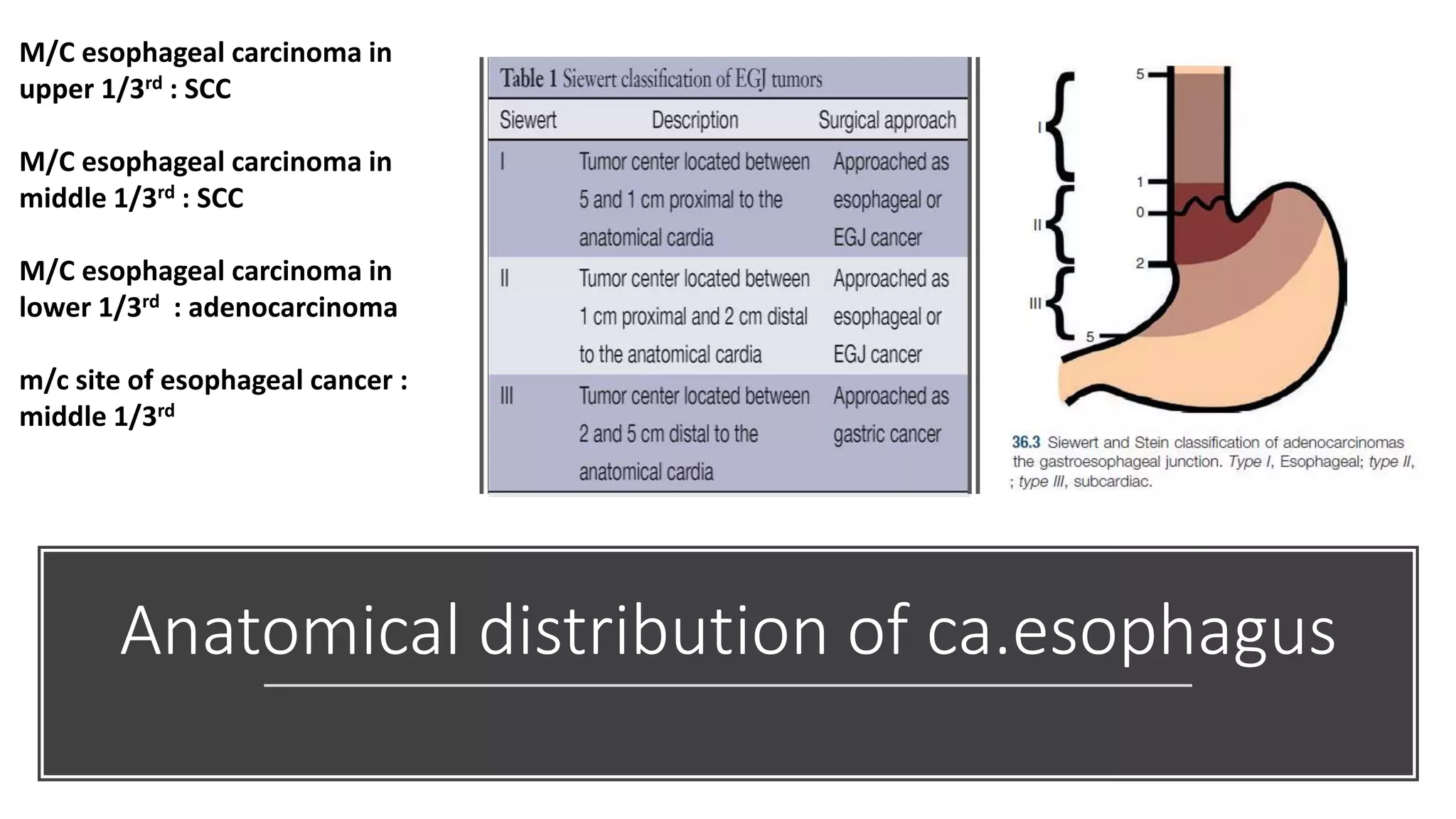

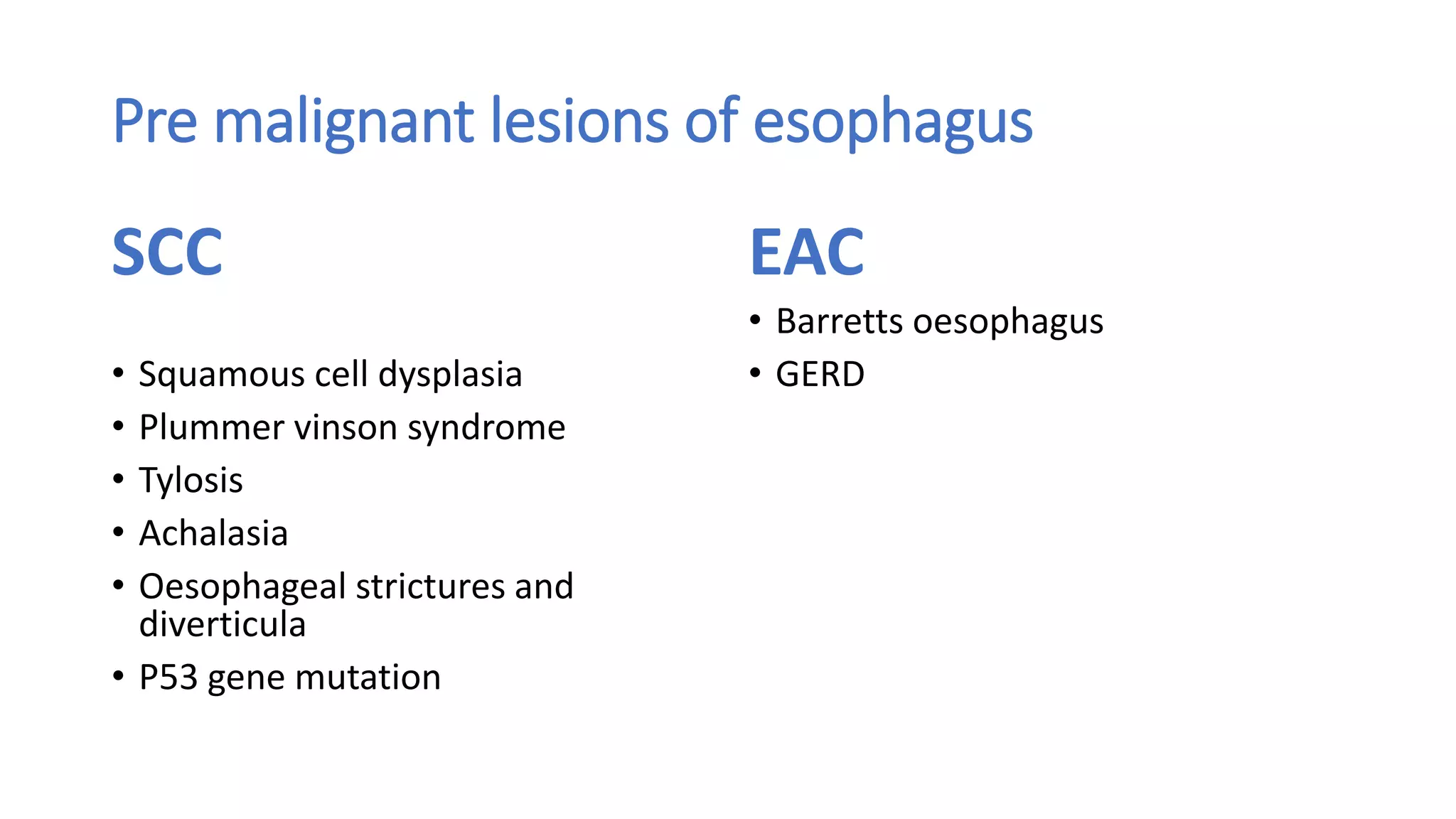













































































This document provides an overview of carcinoma of the esophagus. It discusses the epidemiology, etiology, pathological classification, clinical features, staging, diagnosis and management of esophageal cancer. Esophageal cancer is the 8th most common cancer worldwide and has a poor 5-year survival rate of less than 18%. Risk factors and types of esophageal cancer vary globally. The document outlines the various diagnostic tests and staging systems used to evaluate esophageal cancer as well as endoscopic, surgical and non-surgical treatment options.



































































