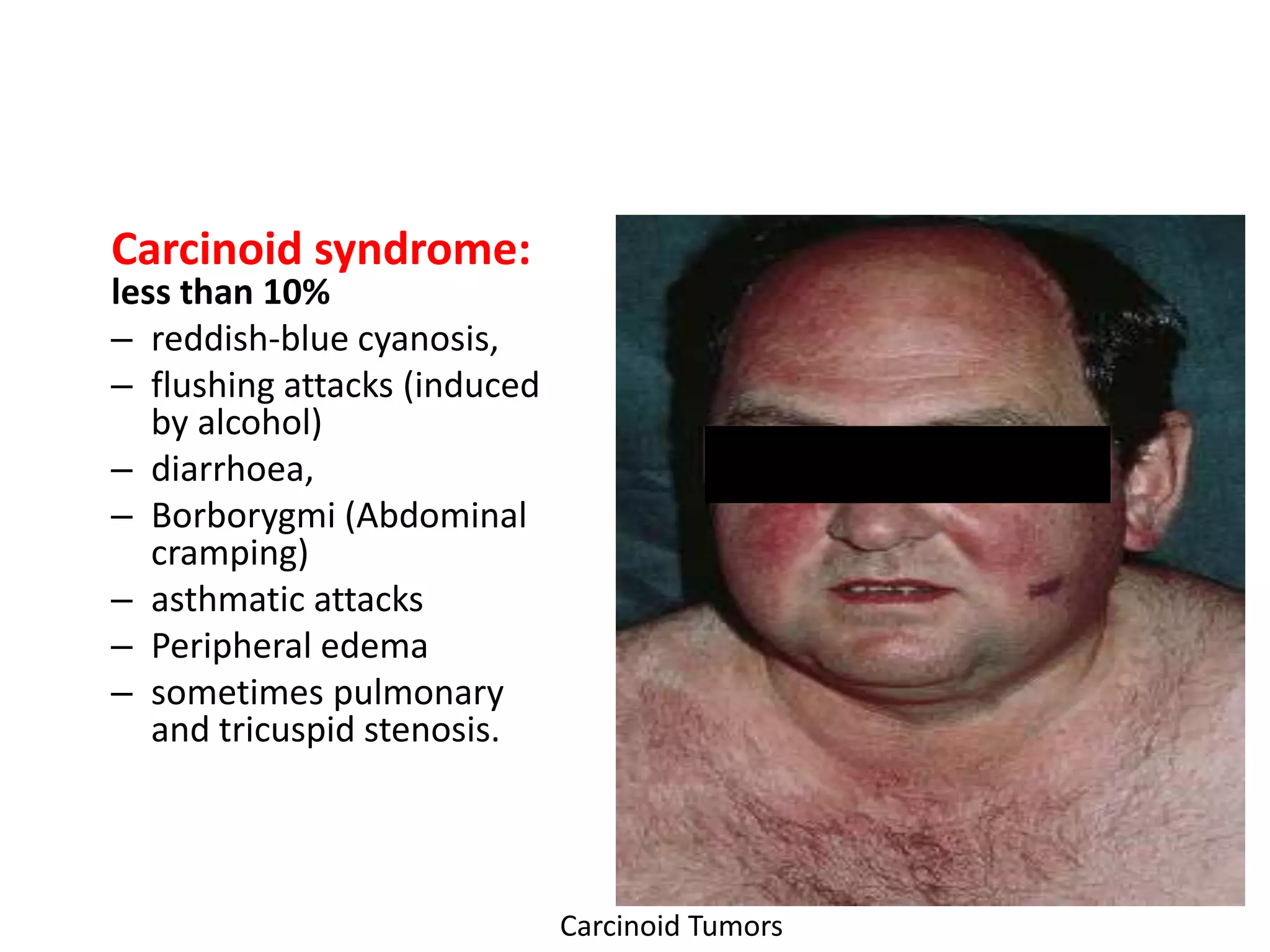
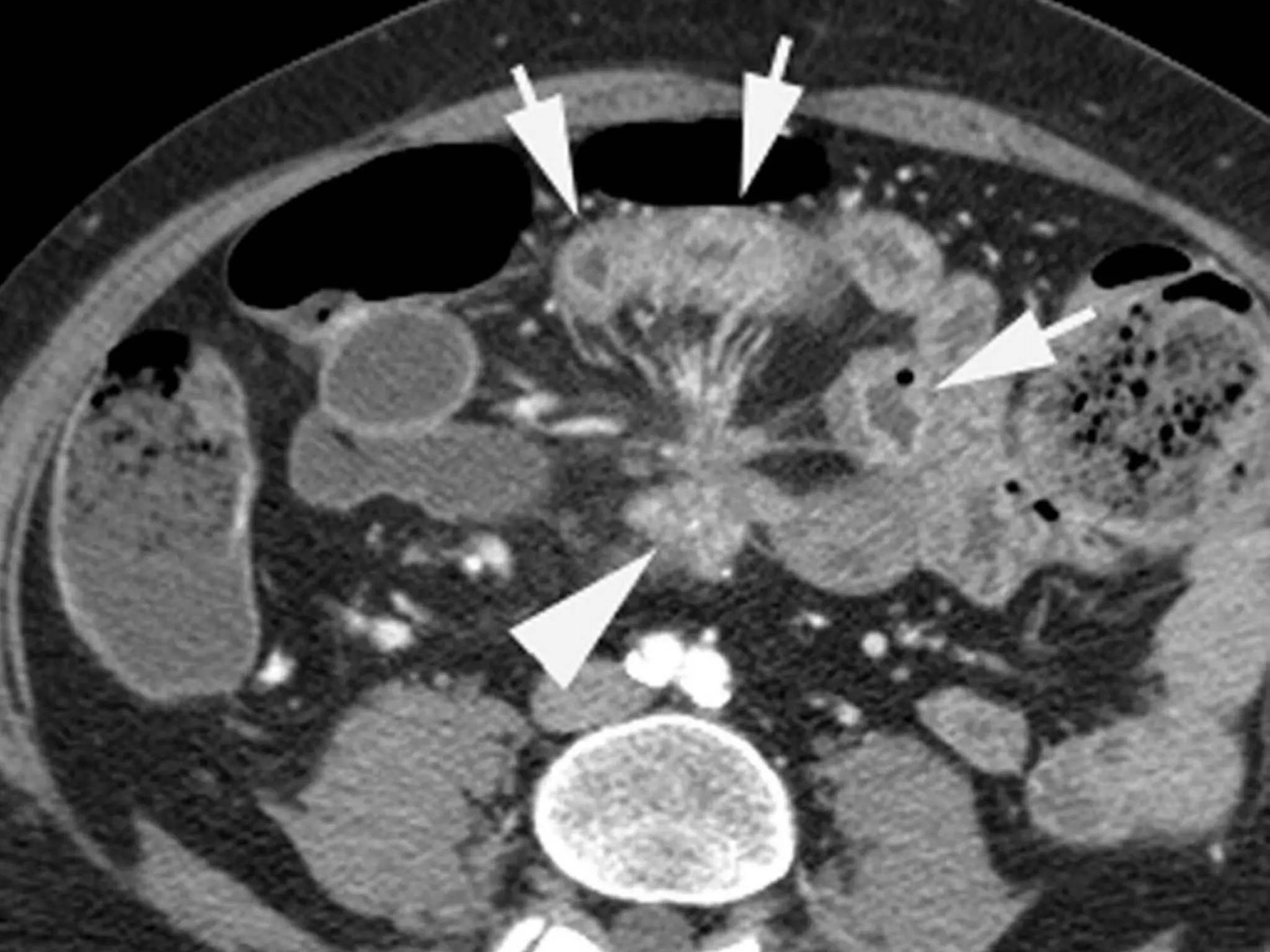

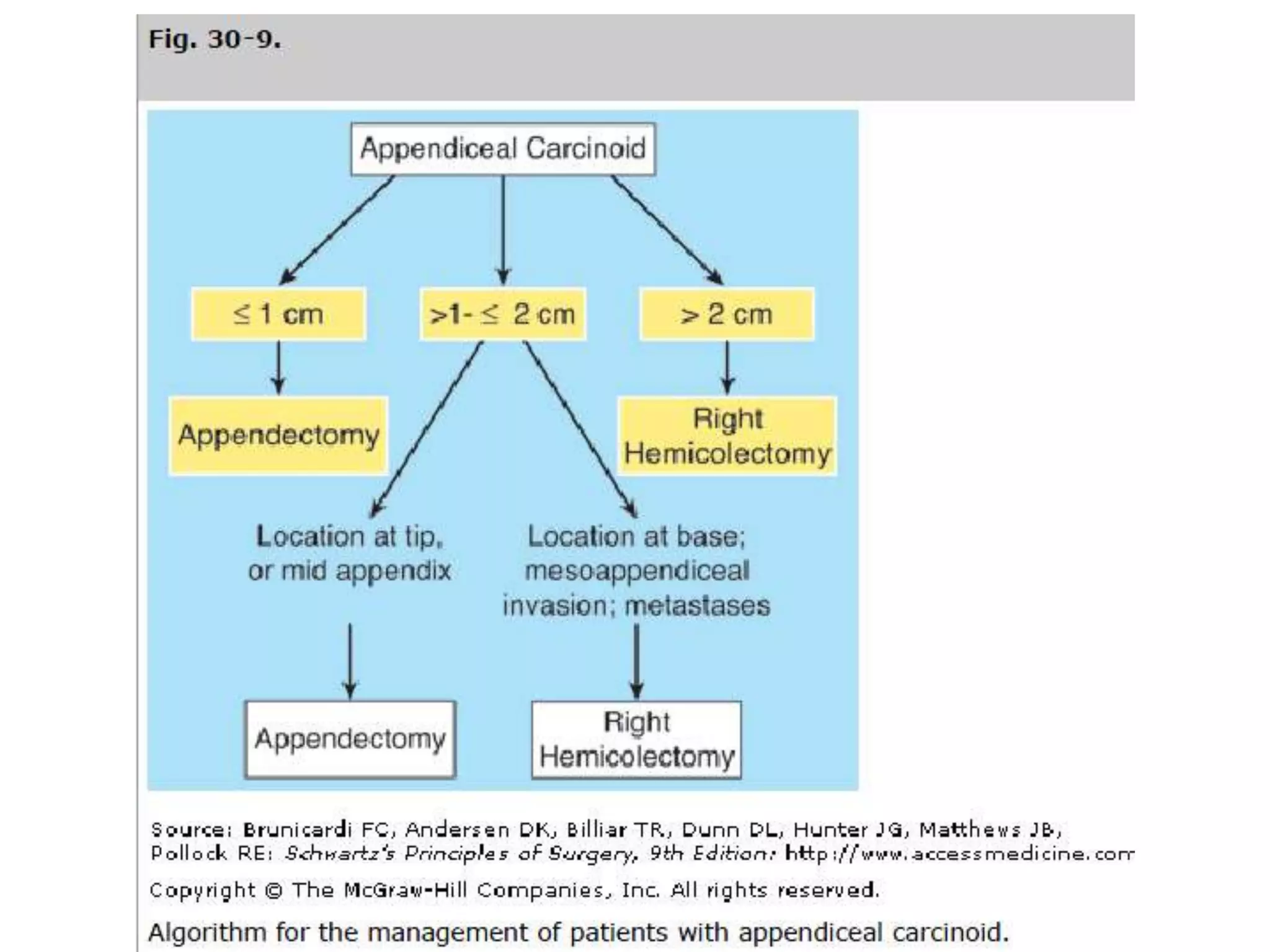

Carcinoid tumors arise from neuroendocrine cells in the gastrointestinal tract. They most commonly occur in the appendix, ileum, and rectum. While often asymptomatic, they may secrete serotonin and cause carcinoid syndrome in rare cases. Diagnosis involves urinary tests for serotonin metabolites and imaging exams. Treatment of localized tumors is surgical resection, while metastatic tumors may also require chemotherapy. Prognosis is generally good if the tumor is localized but worsens with increased size and spread.



































































