Download to read offline

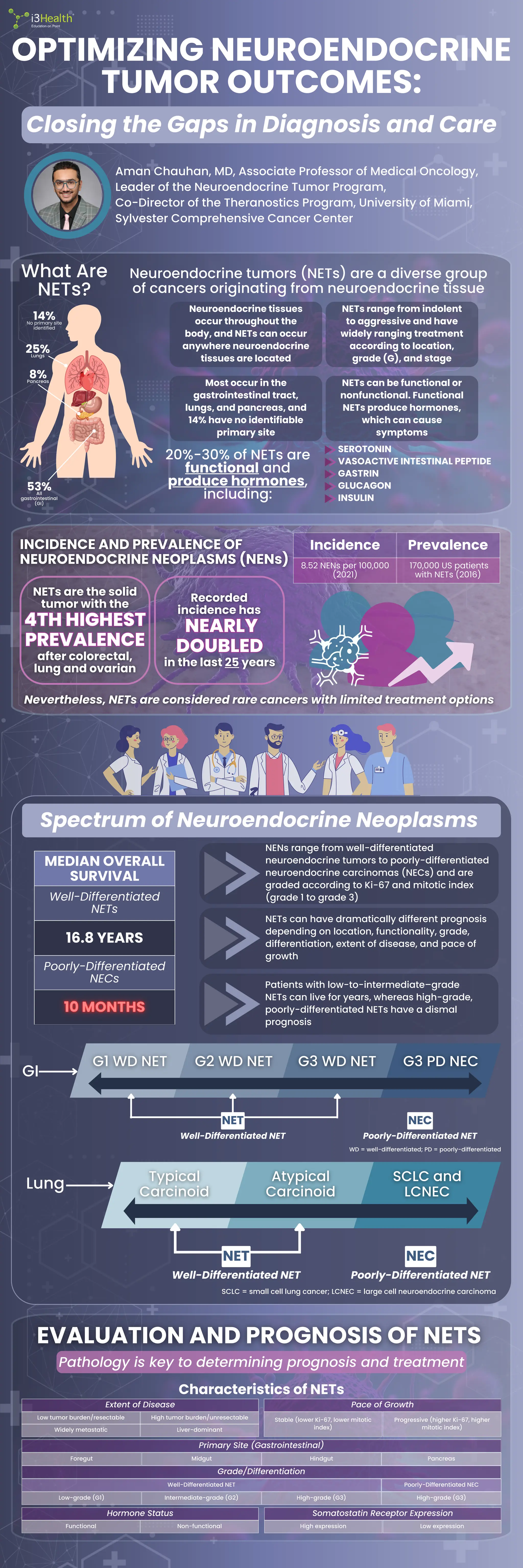
![SYMPTOMS
Abdominal Pain
Nausea
Diarrhea
Indigestion
Weight Loss
Flushing
Persistent Cough
Vomiting
Wheezing
NET patients report having
originally been misdiagnosed
1 in 2
1 in 2
from first symptoms to
correct NET diagnosis
4.3 years
4.3 years
It takes a median of
CORRECT DIAGNOSIS
NETs
NETs
Treatment of NETs
EVALUATION
Imaging
Biochemical
evaluation
Molecular
profiling
Genetic
counseling
Local/
Locoregional
Surgery
Locally
Advanced
Metastatic
Systemic
Therapy
Liver-Directed
Therapy
No role for adjuvant chemotherapy
Immunotherapy
(NECs only)
Chemotherapy
Somatostatin Analogues
Octreotide
Lanreotide
Lu-dotatate
177
Radioligand Therapy
Targeted Therapy
Cabozantinib
Everolimus
Sunitinib
Liver-directed radioembolization
Hepatic arterial embolization
Histotripsy
Liver resection
Thermal ablation
THERAPY
SEQUENCING:
THERAPY
SEQUENCING: Somatostatin
analogues
1
Lu-dotatate
177
(first line for Ki-67 >10%)
2
Cabozantinib, capecitabine/temozolomide
(CAPTEM), everolimus, sunitinib (pNET)
3
1980 1982 1988 2011 2014 2016 2017 2018 2020 2025
SSTR-positive if uptake in
measurable lesions is greater in liver
Ga-dotatate, Ga-dotatoc,
68 68
Cu-dotatate
64
SSTR-PET/CT or SSTR-PET/MRI, or
octreotide SPECT/CT only if SSTR-PET
is not available
Symptoms are
highly variable, from
asymptomatic to
profoundly disabling
Others can cause
mechanical
complications
(bleeding, obstruction)
or hormonal effects
Many NETs are
incidentally
discovered
NETs is a chronic indolent
disease in many
This can be a
not a
Prioritize quality of life
alongside longevity
NETs are
and
Referral to a NET multidisciplinary
program is vital
Accessing a specialized
center is NOT always EASY
Accessing a specialized
center is NOT always EASY
Peptide Receptor
Radionuclide
Therapy (PRRT)
at certain locations
is a significant milestone in NET
treatment, but access can be a
DIAGNOSTIC TOOLS
DIAGNOSTIC TOOLS
Well-Differentiated Poorly-Differentiated
High-grade
(G3)
>20%
>20
High-grade
(G3)
Intermediate-grade
(G2)
Low-grade
(G1)
Grade
Ki-67 Index
Mitotic Index
(mitoses/2 mm )
2
Functional
Imaging
>20%
3%-20%
<3%
>20
2-20
<2
Octreoscan SPECT or SSTR PET-positive
FDG PET-positive
References
Chauhan A, Chan K, Halfdanarson TR, et al (2024). Critical updates in neuroendocrine tumors: version 9 American Joint Committee on Cancer staging system for gastroenteropancreatic neuroendocrine
tumors. CA: A Cancer Journal for Clinicians, 74(4):359-367. DOI:10.3322/caac.21840
Chauhan A, Kohn E & Del Rivero J (2020). Neuroendocrine tumors-less well known, often misunderstood, and rapidly growing in incidence. JAMA Oncol, 6(1):21-22. DOI:10.1001/jamaoncol.2019.4568
Corbett V, Arnold S, Anthony L & Chauhan A (2021). Management of large cell neuroendocrine carcinoma. Front Oncol, 11:653162. DOI:10.3389/fonc.2021.653162
Dasari A, Shen C, Halperin D, et al (2017). Trends in the incidence, prevalence, and survival outcomes in patients with neuroendocrine tumors in the United States. JAMA Oncol, 3(10):1335-1342.
DOI:10.1001/jamaoncol.2017.0589
Dasari A, Wallace K, Halperin DM, et al (2025). Epidemiology of Neuroendocrine Neoplasms in the US. JAMA Netw Open, 8(6):e2515798.
National Comprehensive Cancer Network (2025). Clinical practice guidelines in oncology: Neuroendocrine and Adrenal Tumors. Version 2. 2025. Available at: https://www.nccn.org/guidelines/guidelines-
detail?category=1&id=1448
Oronsky B, Ma PC, Morgensztern D & Carter CA (2017). Nothing but NET: A review of neuroendocrine tumors and carcinomas. Neoplasia, 19(12):991–1002. DOI:10.1016/j.neo.2017.09.002
Perez K, Del Rivero J, Kennedy EB, et al (2025). Symptom management for well-differentiated gastroenteropancreatic neuroendocrine tumors: ASCO Guideline. JCO Oncology Practice, [Online Ahead of Print].
10.1200/OP-25-00133
Singh S, Granberg D, Wolin E, et al (2016). Patient-reported burden of a neuroendocrine tumor (NET) diagnosis: results from the first global survey of patients with NETs. J Glob Oncol, 3(1):34-53.
DOI:10.1200/JGO.2015.002980
Wolin EM, Leyden J, Goldstein G, et al (2017). Patient-reported experience of diagnosis, management, and burden of neuroendocrine tumors. Pancreas, 46(5):639-647. DOI:10.1097/MPA.0000000000000818
This educational activity is supported by a medical education grant from Exelixis, Inc.
GEP-NET = gastroenteropancreatic NET
DIAGNOSIS
DIAGNOSIS PHYSICIAN AWARENESS IS IMPORTANT
PHYSICIAN AWARENESS IS IMPORTANT
If you don’t suspect it, you can’t detect it!
If you don’t suspect it, you can’t detect it!
PATIENT PERSPECTIVES
INCORRECT DIAGNOSIS
Stomach Ulcers
Irritable Bowel Syndrome
Obstructed Bowel
Pneumonia
Gastritis
Asthma
Anxiety or Depression
Menopause
FDG = fluorodeoxyglucose; PET = positron emission tomography; SPECT = single photon emission computed tomography; SSTR = somatostatin receptor; Ga = gallium; Cu = copper
FUNCTIONAL
IMAGING IS KEY
Co-management with a high-volume
multidisciplinary NETs center is highly encouraged
Clinical trials preferred for any line
NEUROENDOCRINE ONCOLOGY
NEUROENDOCRINE ONCOLOGY
ADVANCES IN
ADVANCES IN
Octreotide Lanreotide in
GEP-NET
Telotristat
Ga-Dotatate
PET
68
Streptozocin Everolimus
Sunitinib in
pNET
Everolimus
in Lung/GI NET
Capecitabine/
Temozolomide
Lu-Dotatate
177
Cu-Dotatate PET
64
Cabozanitinib
pNET = pancreatic neuroendocrine tumor
Lu = lutetium
Targeted therapies
(cabozantinib,
everolimus) are effective
but can have side effects
and
are key](https://image.slidesharecdn.com/245nets-infographic-251014010943-b5b086f7/85/Infographic-Optimizing-Neuroendocrine-Tumor-Outcomes-2-320.jpg)

i3 Health is pleased to make the speaker slides from this activity available for use as a non-accredited self-study or teaching resource. Neuroendocrine Tumors are tough to spot, tougher to treat. This infographic, created from Aman Chauhan, MD, Associate Professor of Medical Oncology, Leader of the Neuroendocrine Tumor Program, and Co-Director of the Theranostics Program at the University of Miami, Sylvester Comprehensive Cancer Center, presentation, delivers the latest diagnostic breakthroughs, treatment options, and personalized care strategies to improve patient outcomes. Get the insights you need, now! STATEMENT OF NEED Neuroendocrine tumors (NETs) are a heterogeneous group of rare tumors that originate from epithelial or nervous cells in the neuroendocrine system. They can arise from any organ, most commonly the gastrointestinal tract and lungs. Clinical presentation of NETs is highly variable, and patients can experience a broad spectrum of symptoms that significantly impact well-being and make diagnosis challenging. The last decade has seen progress in therapy for NETs based on improved pathological categorization and molecular understanding, resulting in increasing therapeutic choices. Therefore, it is crucial for clinicians to remain up to date on emerging diagnostic techniques and therapies to improve outcomes for their patients with NETs (Sultana et al, 2023). This actlvity, presented by Aman Chauhan, MD, Associate Professor of Medical Oncology, Leader of the Neuroendocrine Tumor Program, and Co-Director of the Theranostics Program at the University of Miami, Sylvester Comprehensive Cancer Center, will explore strategies for optimizing NET outcomes by closing the gaps in diagnosis and care. TARGET AUDIENCE Medical/radiation/surgical oncologists, pathologists, endocrinologists, gastroenterologists, advanced practice providers, and other healthcare professionals (HCPs) involved in the treatment of patients with neuroendocrine tumors (NETs). LEARNING OBJECTIVES Recognize the diverse clinical presentations of NETs to enhance differential diagnosis skills Identify patients at high risk for recurrence based on disease-related factors and patient characteristics Develop guideline-concordant, personalized treatment plans for patients with NETs, incorporating insights from recent clinical trials of novel therapies Relevant financial relationships exist between the following individuals and ineligible companies: Aman Chauhan, MD, discloses that he has served on an advisory board or panel for Boehringer Ingelheim, Curium, Exelixis, Novartis, Sanofi, and Seneca Therapeutics. The i3 Health planners, reviewers, and managers have nothing to disclose. i3 Health has mitigated all relevant financial relationships. COMMERCIAL SUPPORT This educational activity is supported by a medical education grant from Exelixis, Inc. Aggregate participant data will be shared with commercial supporters of this activity



































































