
More Related Content
What's hot
What's hot (20)
Similar to Pathology NET.ppt
Similar to Pathology NET.ppt (20)
More from Nirupama kothari
Recently uploaded
Recently uploaded (20)
Pathology NET.ppt
- 2. Neuroendocrine System • Dispersed system of cells present in the CNS, PNS and in many organs including classic endocrine organs, the gut, pancreas, lung, etc.
- 3. What is a Neuroendocrine Cell? • “Neuroendocrine” defines the peptide hormone – producing cells • These cells have in common the ability for Amine Precursor (viz. DOPA and 5 OH tryptophan) Uptake and Decarboxylation - APUD cells
- 4. Definition of NET • Neuroendocrine tumors (NET) are neoplasms which produce and secrete glycopeptide hormones and biogenic amines and share neural – endocrine markers. • GEP – NET most common of all NET’s • Homogenous in terms of morphology but are heterogeneous in terms of biological and clinical features Bosman FT, et al. WHO Classification of Tumors of the Digestive System.Lyon, France: IARC Press;2010.
- 5. Gastroenteropancreatic Neuroendocrine Tumor • Standardized histopathological diagnosis and classification on biopsy or surgical specimen - basis for prognostic stratification, for optimal selection of the respective tumor specific imaging procedure and therapeutic option.
- 6. Nomenculature issues 1. Endocrine Vs Neuroendocrine Neoplastic cells have features of neural and epithelial cells. WHO recommended term – Neuroendocrine. 2. Tumor vs neoplasm Tumor = mass Neoplasm = acurate Widespread acceptance in many systems – Neuroendocrine tumor (NET).
- 7. 3. Carcinoid tumor Term does not adequately convey the potential for malignant behavior that accompanies many of these neoplasms. However this term retains widespread colloquial usage. Nomenculature issues
- 8. How to diagnose NET
- 9. Neuroendocrine Cell Small Synaptic vesicle Synaptophysin expression Neurosecretory granule with peptide secretion Chromogranin A at NSG membrane N Blood (Tumor diameter is 3mm) Biomarkers
- 10. Blood biomarkers Chromogranin A (CgA) • Sensitivity: CgA 78 – 84% • Specificity : CgA 71 – 85% • False positive - Renal insufficiency - Hypertension - PPI Zatelli MC, et al., Endocr Relat Cancer.2007;14(2):473-482
- 11. Tissue Diagnosis: FNAC vs Core Biopsy Core Biopsy • More tissue • Higher comfort level to diagnose malignancy • IHC for diagnosis and grading
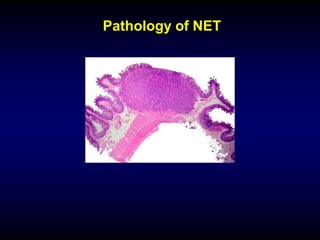
- 12. Diagnosis of NET • Monotonous small round cells with uniform nuclei, stippled chromatin (salt and pepper)
- 13. In 1971 Soga and Tazawa described 4 microscopic patterns: 1. Insular (nodular solid nests with peripheral invading cords) NET - Microscopic Patterns
- 14. 2. Trabecular (anastomosing trabeculae or ribbons) NET - Microscopic Patterns
- 15. 3. Glandular (tubules, acini or rosettes) NET - Microscopic Patterns
- 16. 4.Poorly differentiated with no well - organized growth pattern NET - Microscopic Patterns
- 17. Markers of neuroendocrine differentiation – IHC Non Hormonal Markers • Chromogranin- acidic proteins in secretory granules. Type A, B, C • Synaptophysin • NSE • PGP9.5, CD57, CD56, VMAT2 Hormonal markers – Gastrin (G cells), Somatostatin (D Cells), Serotonin (E cells), Glucagon (L cells) Calcitonin CgA Synap
- 18. Role of CgA in Dx of NET Benefits • Integral part of the membrane of neurosecretory hormone granules • Can be detected in the secretory granules of most NET, both symptomatic and asymptomatic Taupenot L, Harper KL, O’Connor DT.N Engl J Med.2003;348:1134-1149
- 19. Role of CgA in Dx of NET Limitations: • Many NET of the large bowel and some of the appendix primarily secrete CgB • Dependent on no.of neurosecretory vesicles / cell • CgA may be negative in poorly differentiated NET
- 20. Role of Synaptophysin in Dx of NET Benefits: • Expressed independently of secretory granules • Useful in identifying poorly granulated and poorly differentiated NET that may not exhibit CgA Chetty R et al. Arch.Pathol Lab Med 2008;132:1285-1289 Limitations: • Expression is not limited to neuroendocrine cells
- 21. Unknown primary • For metastatic GEP-NET with unknown primary evidence of specific transcription factors in addition to hormones is important.
- 23. Islet 1 (IsI1) expression is a reliable marker for pancreatic neuroendocrine tumors and their metastases1 Liver mts IsI1 1.Schmitt AM et al.Am J Surg Pathol.2008 Mar;32(3):420-5. PNET – has liver / LN mets by the time of diagnosis
- 24. CDX2 as a marker of intestinal EC-cells and related well-differentiated neuroendocrine tumors1 1. La Rosa S et al Virchows Arch.2004 Sep;445(3):248-54 CDX2 1. CDX2 - Positive in 90% of NET of ileum and appendix but not in pulmonary NET 2. TTF -1 is expressed in 50% of bronchopulmonary NET but only <2% of GEP - NET
- 25. Stomatostatin Receptors • Somotostatin receptor (SSTR) are expressed on the surface of Neoplastic Neuroendocrine cells • 5 types of SST receptors • SSTR 2A has greatest binding affinity to somatostatin analogues
- 26. sstr2 in NETs • Almost 40% of the patients with NET have very strong staining for sstr2 Missiaglia E, et al. J Clinic Oncol.2010, 28(2):245-255
- 27. SSTR IHC: 77% correlates with Octreotide Scintigraphy 107 Cases (41 pre-operative samples) Volante M.et al Mod Pathol.2007 Nov;20(11):1172-1182
- 28. Functionality issue of NET • Functional NETs - defined based on the presence of clinical symptoms due to excess hormone secretion by the tumor • Functional status of the tumor is defined by clinical findings and not by pathologic appearance or IHC profile (eg: carcinoid syndrome) • Non functional NET’s – associated with symptoms related to mass
- 29. • Pathologic diagnosis of functioning NETs should be the same as for analogous nonfunctioning NETs of the same anatomic site, with the descriptive functional designation appended to the diagnosis when there is knowledge of a clinical syndrome. Functional status need not be included in the pathology report Functionality issue of NET
- 30. 0 24 48 72 96 120 0 24 48 72 96 120 Cumulative Survival Probability Cumulative Survival Probability Time of survival (months) Time of survival (months) Impact of histology, proliferation, & stage on prognosis. P-NEN St.l (108 pts) St.ll (16 pts) St.lll (54 pts) St.lV (96 pts) 0 – 5% (152 pts) >5 – 20% (63 pts) >20% (22 pts) Ki 67 levels 0 24 48 72 96 120 Cumulative Survival Probability Time of survival (months) WDET-B (51 pts) WDET-U (56 pts) WDEC (139 pts) PDEC (28 pts) WHO 2000 classification TNM coding Scarpa et al Mod Pathol 2010
- 31. NENs, NETs, NECs & MANECs of the GEP Comparison of Classifications Bosman FT, et al. WHO Classification of Tumours of the Digestive System. Lyon, France: IARC Press; 2010. WHO 1980 WHO 2000 WHO 2010 Carcinoid WDET- Benign Uncertain WDEC PDEC/ SCC NET G1 NET G2 NET G3 NEC G3 Mucocarcinoid Mixed carcinoid and adenoca Mixed exocrine endocrine carcinoma (MEEC) Mixed adeno- neuroendocrine carcinoma (MANEC) Pseudotumour lesions Tumour-like lesions Hyperplastic and preneoplastic lesions
- 32. WHO 2010 Update Classification, Staging, Prognosis Working principles – New classification – retains basic criteria of WHO 2000 classification – All GI NET’s have a malignant potential – Separation of histological grading & staging parameters – “Neuroendocrine neoplasm/tumor” includes well and poorly differentiated tumors – Benign & low malignant highly diff NET – jointly referred as Neuroendocrine tumors (G1(synonym for carcinoid) & G2) – Well differentiated NET – G1,G2,G3 – Neuroendocrine Carcinoma – All poorly differentiated NET – G3(small cell & large cell NEC)
- 33. NET – Tumor differentiation by histology
- 34. Well differentiated NET - Histology • Well - differentiated tumors have characteristic organoid arrangement of the tumor cells, with nesting, trabecular or gyriform patterns. • Cells are uniform and produce abundant neurosecretory granules, reflected in the strong and diffuse immunoexpression of neuroendocrine markers Cg A and synaptophysin.
- 35. Poorly differentiated NET - Histology • Poorly differentiated NETs less closely resemble non- neoplastic neuroendocrine cells and have a more sheetlike or diffuse architecture, irregular nuclei, and less cytoplasmic granularity. • Immunoexpression of neuro-endocrine markers is usually more limited.
- 36. Can pathologists provide predictive markers? In a well or moderately differentiated NET, even in the absence of a positive octreoscanTM , somatostatin analogue therapy can have benefit 1. Zatelli MC et al. Horm Metab Res.2003.35(6):349-354; 2. Vezzosi D et al. Clin Endocrinol (Oxf).2008,68(6): 904-911; 3. Vezzisi D et al.Eur J Endoscrinol.2005, 152(5):757-467. Differentiation of well differentiated from poorly differentiated NET is the most important pathological assessment as therapy defers
- 37. Grade versus differentiation of NET Differentiation Grade Well differentiated Low grade G1 – relatively indolent Intermediate grade G2 - moderately aggressive High grade G3 – ext aggressive Poorly differentiated High grade G3 – ext aggressive •Grade refers to the inherent biologic aggressiveness of the tumor. The proliferative index is inherently linked to the grade of NET
- 38. Mitotic Count • The simplest method to determine the proliferative index is to count mitotic figures, and is necessary for complete pathology reports. • The mitotic rate should be expressed based on the number in 10 high power fields (2 mm2) • A total of 50 fields (10 mm2) should be counted
- 39. Grading by Mitotic Counts Rindi G et al. Circhows Arch (2007) 451:757 – 762 American Joint Committee On cancer.AJCC Cancer Staging System.Seventh Edition
- 40. Ki 67 widely used Europe than in US
- 41. Ki67 Counting • Options to quantify Ki67 Systematically counting manually a defined number of tumors cells (500 – 2000) and calculating the positive percentage Using a computerized digital image analysis system to measure the positive percentage A general “eyeballed” estimate of the percentage of positive cells • Proliferative rate - Provides significant prognostic information for NET.
- 43. Ki 67 Cell block / Biopsy - Impossible to count mitotic figures in 40 – 50 / hpf. Limited tumor tissue Ki67 staining - more accurate
- 44. Grading of NET According to Ki67 index The result should be reported as a single percentage, reflecting the average of the regions counted, rather than a range of values.
- 45. 2010 WHO GI NET Grading by Mitotic Counts vs Ki-67 G1 G2 G3 Morphology low grade low grade high grade H & E Mitotic count <2 2 - 20 >20 (10 HPF) IHC Ki67 index <2 3 – 20 >20 (% of positive cells per 100 counted cells)
- 46. Mib 1 Ki67 WD G3 G3 – high grade malignant behavior >20%
- 47. MANEC • Carcinoma phenotype that is recognizable as both adenocarcinoma and neuroendocrine carcinoma • Each component exceeds at least 30% of all neoplastic cells • Both components should be graded • The identification in adenocarcinomas of scattered neuroendocrine cells (<30%) does not qualify for MANEC
- 48. Staging issues • American Joint Committee on Cancer (AJCC) – Anatomic site specific TNM staging for NETs • European Neuroendocrine tumor society (ENETS) (2006, 2007) • Considerable over lap with some differences between these two • For Appendix & Pancreas – use both ENETS & AJCC TNM staging as they differ in definitions of T stages of tumor
- 50. NET - Minimum Pathology Data Set • Diagnostic term • Anatomic site of tumor • Size (3 dimensions) • Tumor histopathology • Morphology, extent of invasion (T) IHC staining, multicentric disease, non-ischemic tumor necrosis, vascular invasion, perineural invasion, lymph node metastases (total no/ number positive - N) • Proliferative activity grade (mitotic rate, Ki67 index) • TNM staging (specify staging used) • Resection margins (positive/negative/close) Am J Surg Pathol; 2010:34;300-313
- 51. SUMMARY • All GEP NET’s are of low grade malignant potential • Use WHO 2010 classification • Evidence of neuroendocrine nature of the tumor (morphology & IHC for neuroendocrine markers) • Histological distinction between well and poorly differentiated tumors • Proliferation based grading (Ki67 mandatory for grading (G1,G2,G3) • PTNM staging with reference of specific system used
Editor's Notes
- 11
- 17
- 46