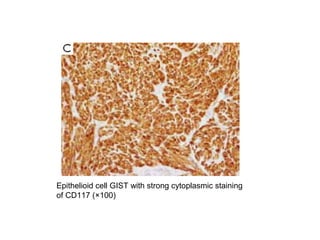
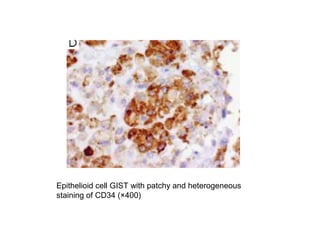
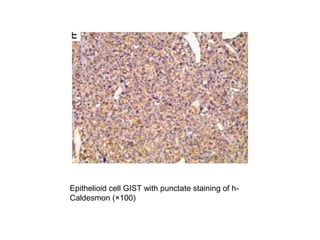
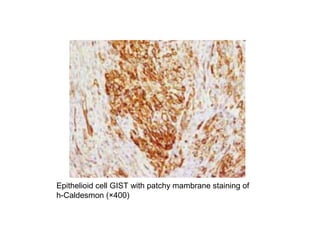
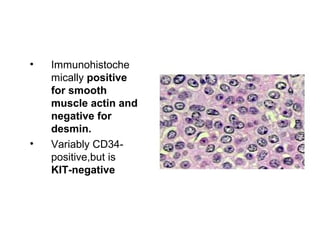
Gastrointestinal stromal tumors (GISTs) arise from interstitial cells of Cajal in the gastrointestinal tract. Pathogenic mutations in KIT or PDGFRA genes drive tumor growth in most GISTs. GISTs most commonly occur in the stomach and small intestine. Microscopically, GISTs demonstrate spindle or epithelioid cell morphologies and strongly express KIT (CD117). Surgical resection is the primary treatment, while the tyrosine kinase inhibitor imatinib is effective for advanced or metastatic disease. Tumor size, mitotic rate, and site determine prognosis, with small intestinal GISTs having the worst outcomes.