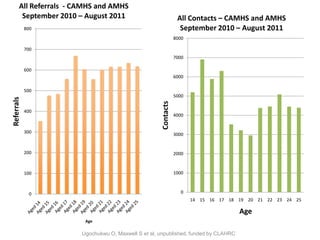


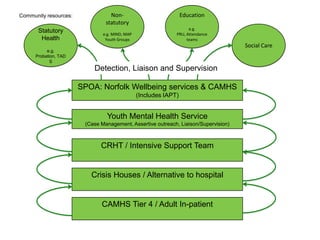





This document summarizes the development of a dedicated youth mental health service in Norfolk. Key points include collaborating with young people, clinicians, and commissioners to address gaps in services between child and adult mental health. A pilot program was launched in 2012 to engage those at highest risk aged 14-25 through a range of medical, social, and vocational interventions to prevent admissions. Outcomes and further research were planned to evaluate prevention of long-term social disabilities. Challenges included gaining buy-in from all stakeholders and securing necessary resources.























































































