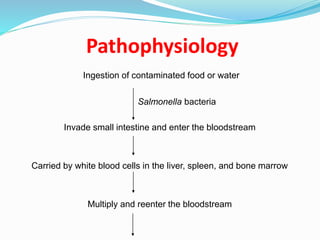
Typhoid fever is caused by the Salmonella Typhi bacteria. It is transmitted through contaminated food or water. Symptoms include sustained high fever, weakness, abdominal pain, and headaches. Diagnosis involves blood, stool, or urine cultures. Treatment consists of antibiotics like chloramphenicol or ciprofloxacin for 10-14 days along with rest and proper nutrition. Prevention relies on proper sanitation, hygiene, and vaccination.