Download to read offline






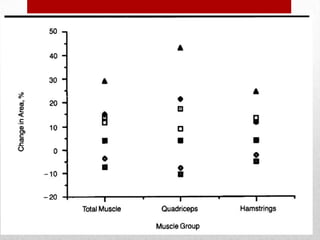

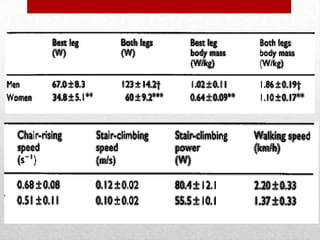
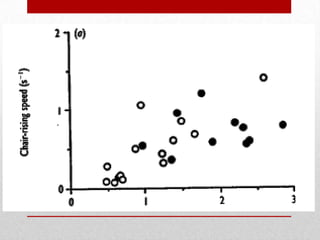
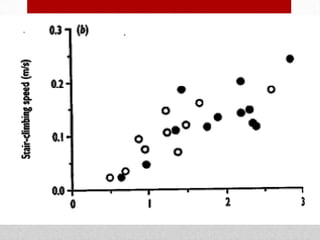
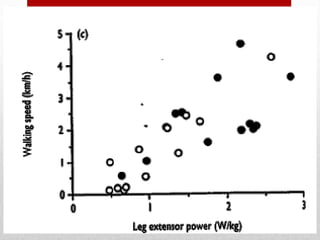
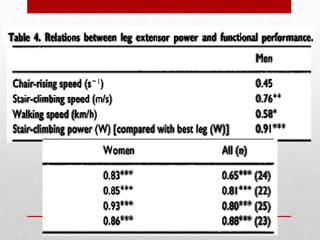


This document summarizes two studies on aging research at Tufts University. The first study found that high-intensity strength training significantly increased muscle strength in nonagenarians (people in their 90s) living in a long-term care facility, with some participants showing functional improvements. The second study found that leg extensor power, a measure of muscle strength and speed, predicted performance on tasks like chair rising, stair climbing, and walking in very old adults, and identified gender differences and thresholds related to independence. Both studies demonstrated the feasibility and benefits of resistance training for frail elderly populations.











































































