Downloaded 100 times





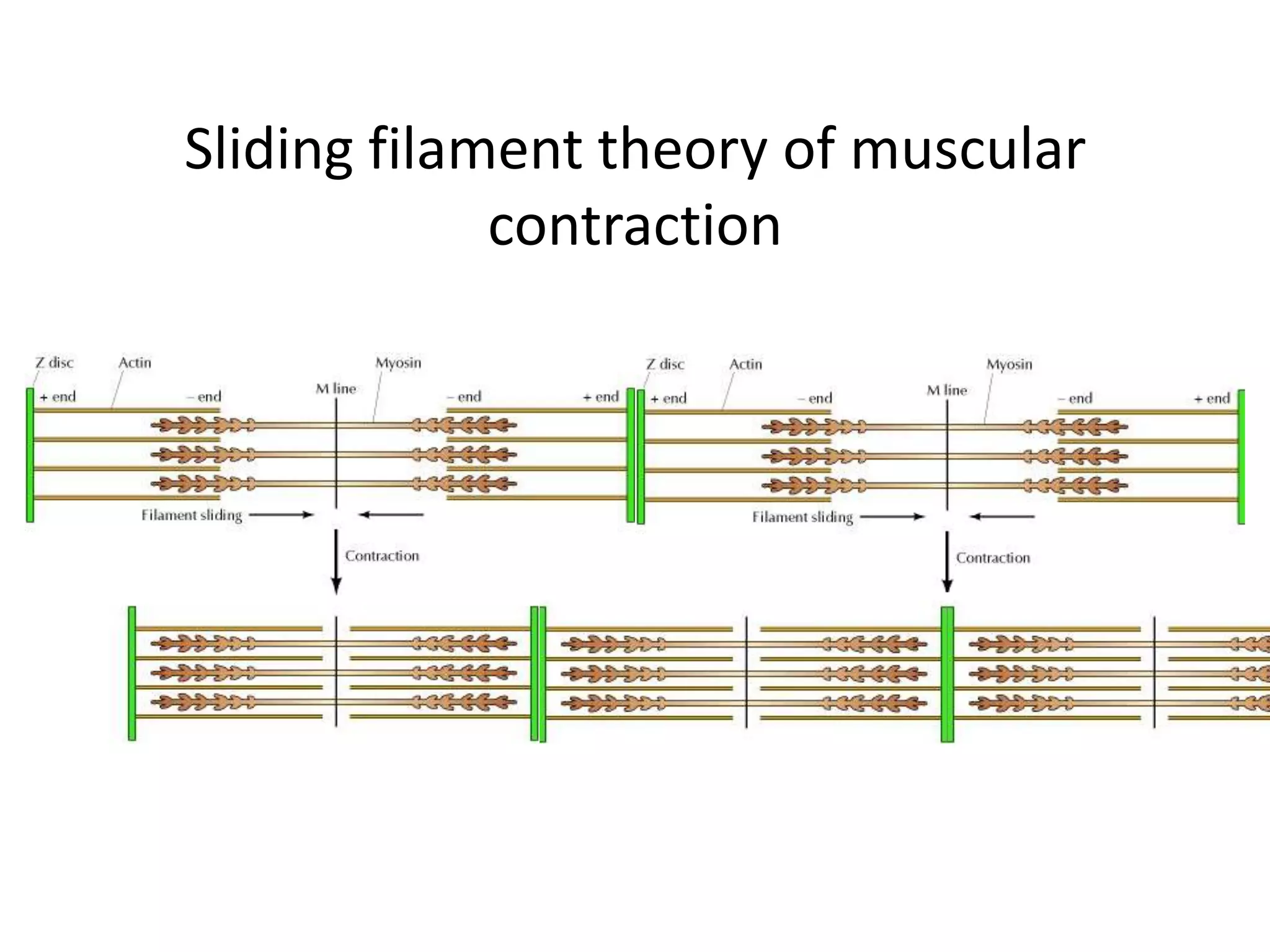













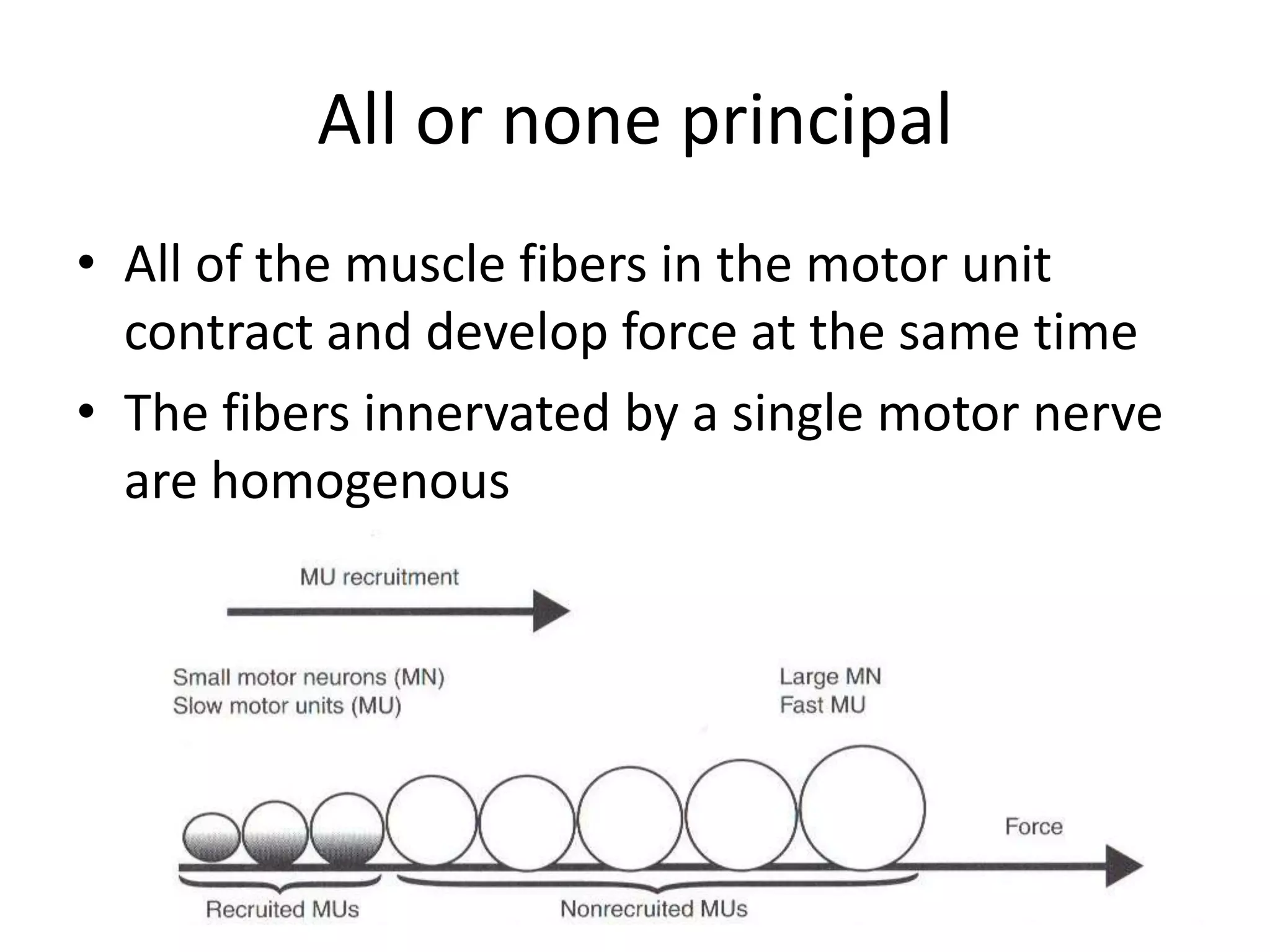
































The document discusses skeletal muscle physiology, types of muscle fibers, and the impact of training and aging on muscle performance. It highlights the importance of specific training protocols for different muscle types and concludes with insights into aging muscle and associated interventions for older adults. Additionally, it addresses research opportunities in the context of muscle function and various health conditions, including cystic fibrosis.























































































