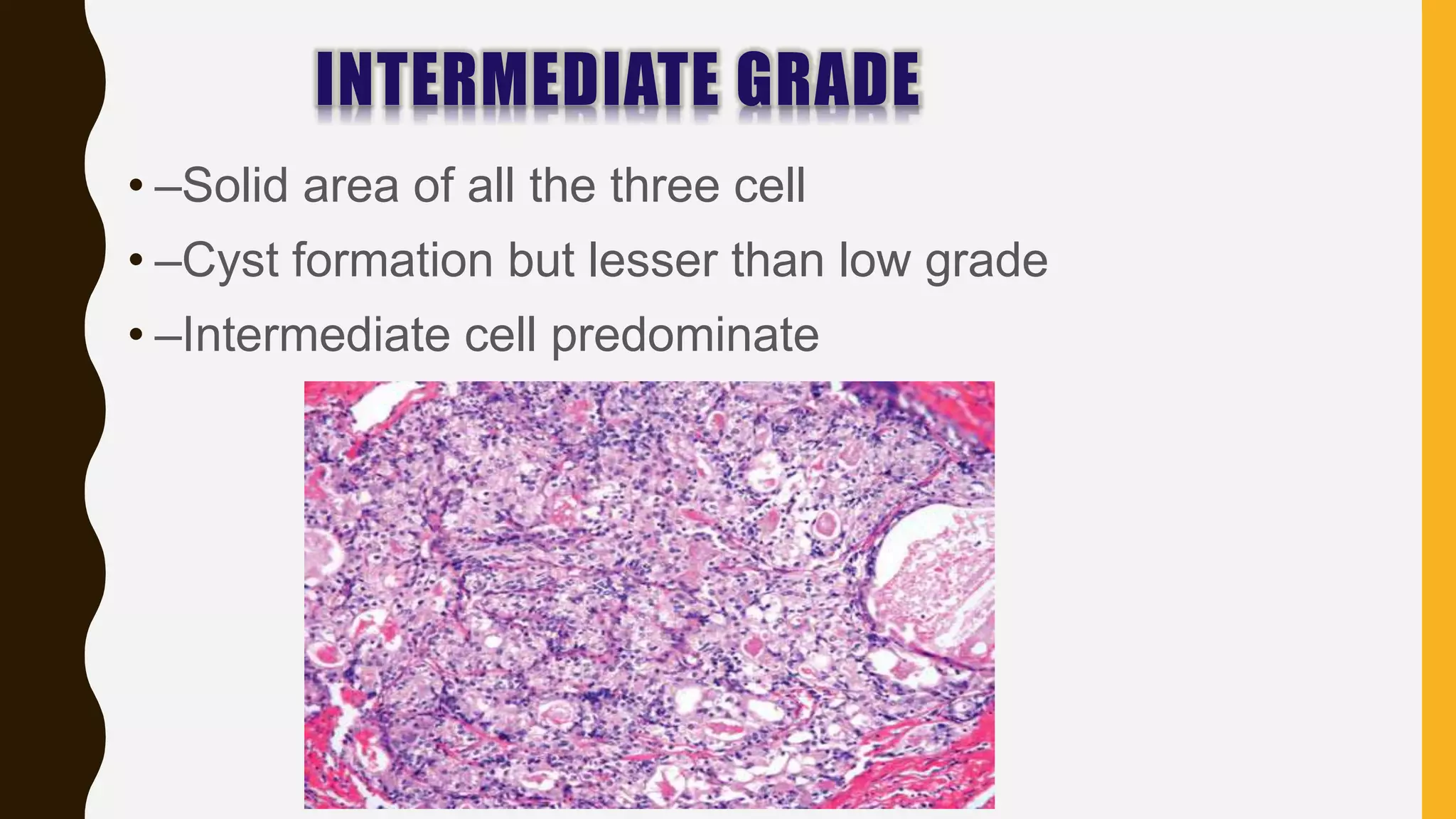
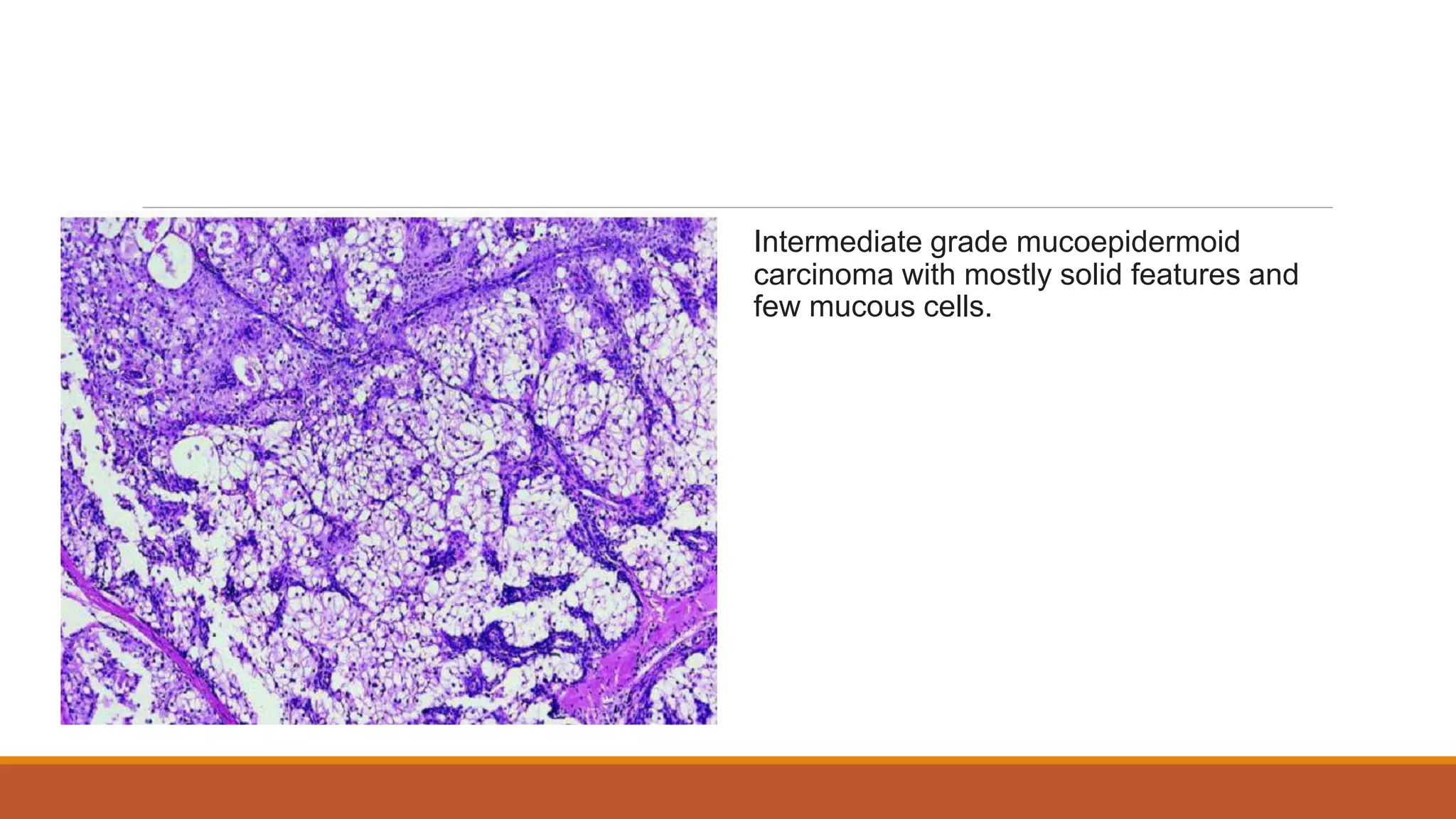
Mucoepidermoid carcinoma is a malignant glandular epithelial tumor that contains both epidermoid and mucus-secreting cells. It most commonly arises in the parotid gland but can also affect minor salivary glands. Histologically, it is graded based on the degree of cyst formation, cellular atypia, and relative numbers of the three cell types. Low grade tumors have many mucus cells and cysts while high grade tumors are more solid with necrosis and invasion. Treatment involves surgical excision with radiation and chemotherapy possibly added for advanced or high grade disease. Prognosis depends on grade, with low grade having over 90% 5-year survival versus intermediate and high grade around 50%.