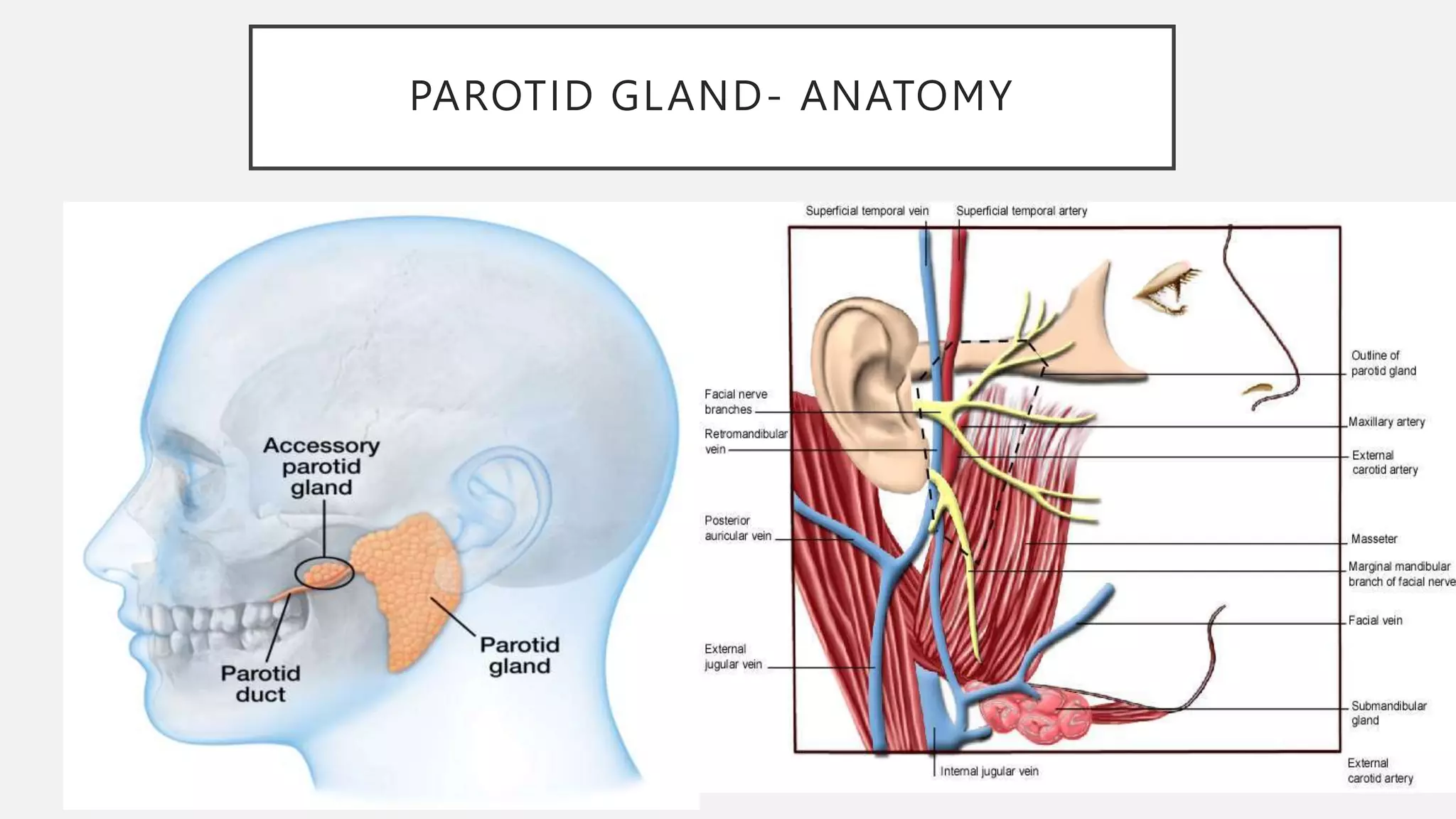
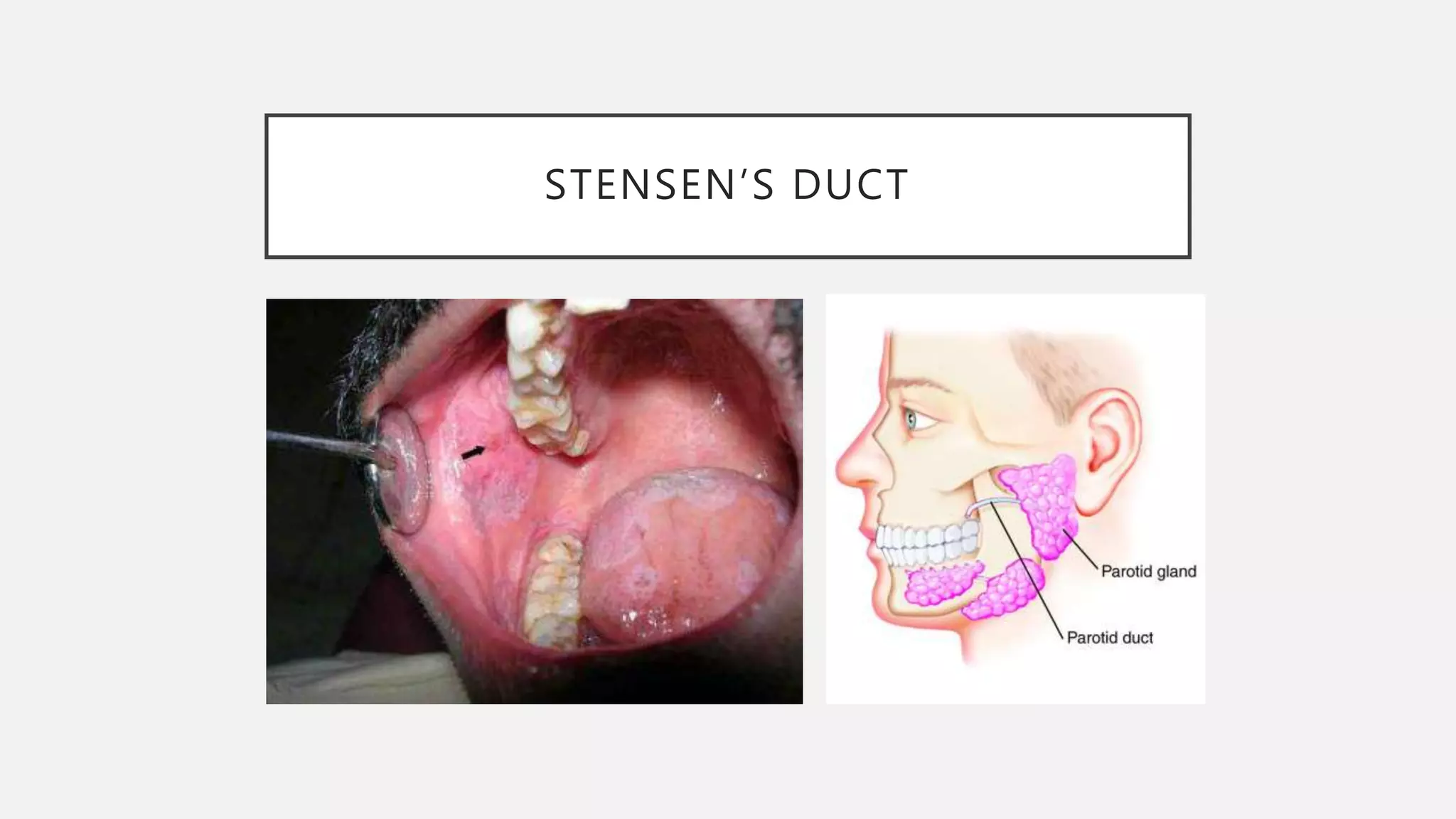
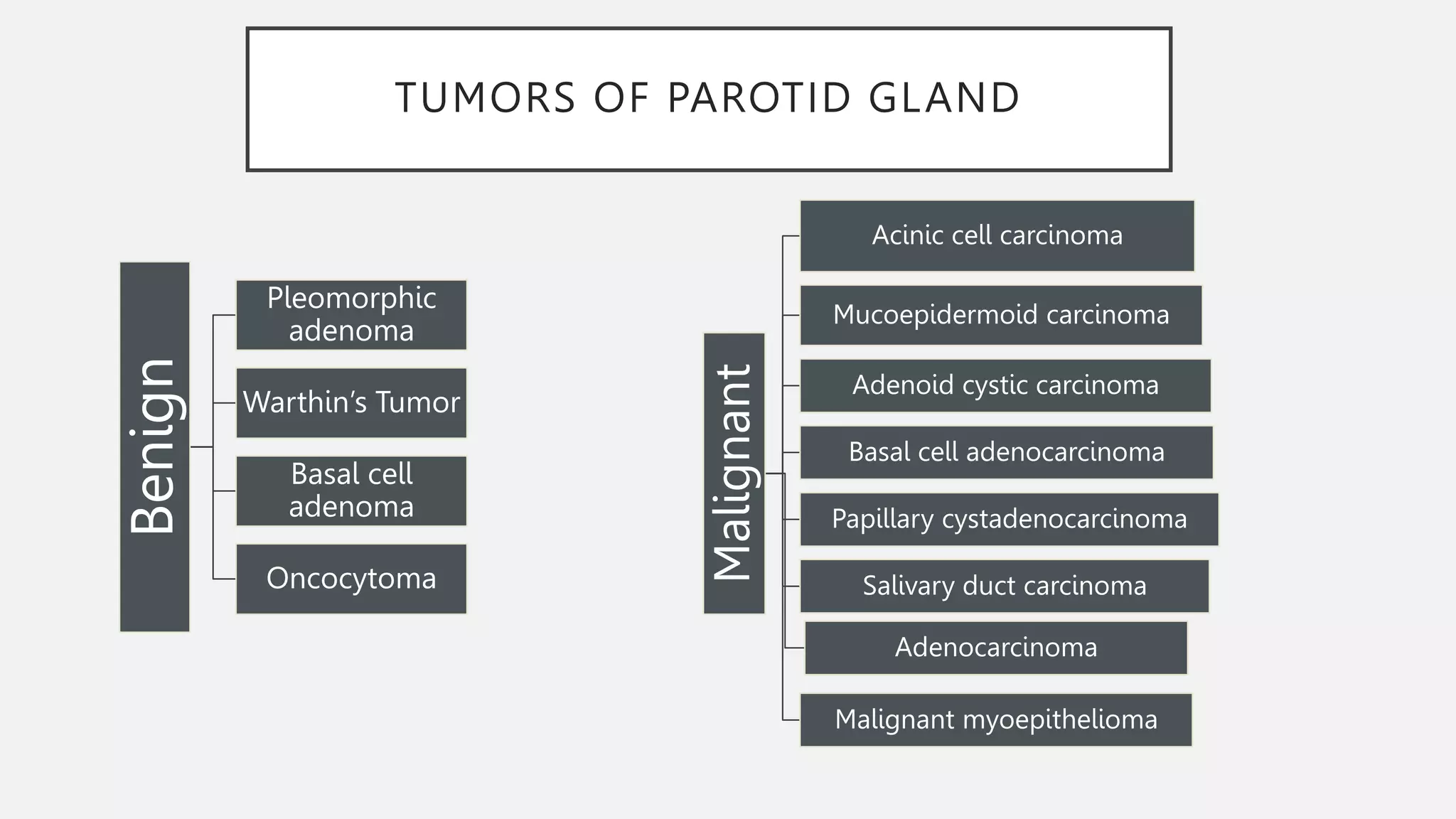
The document discusses the anatomy of the parotid gland. It describes the parotid gland as being located in the retromandibular fossa, weighing 15-30 grams, and having superficial and deep lobes. It notes the parotid gland's relationship to critical head and neck structures. The document also discusses Stensen's duct, arteries and veins related to the parotid gland, the facial nerve's course through the gland, lymph nodes that drain the gland, and common conditions and tumors that affect the parotid gland.