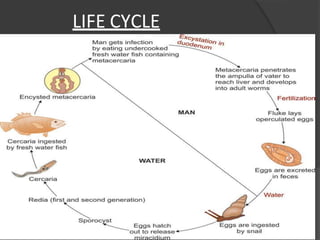
The document provides an extensive overview of various trematodes (flukes), detailing their morphology, life cycles, pathogenicity, clinical features, and diagnostic methods. Specific species discussed include Schistosoma haematobium, Schistosoma mansoni, S. japonicum, Fasciola hepatica, and others, emphasizing their habitats, infections, and treatments. The document outlines preventive measures and treatment options, primarily focusing on praziquantel as the drug of choice.





















































![[Micro] hymenolepis nana](https://cdn.slidesharecdn.com/ss_thumbnails/3rxjz7ekrwinb1sq3uxs-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)