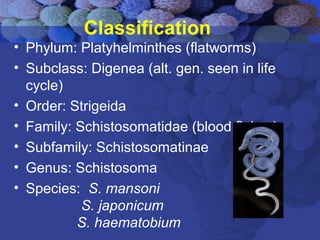
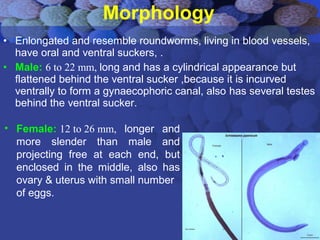
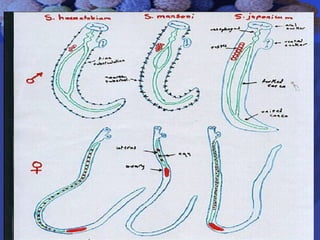
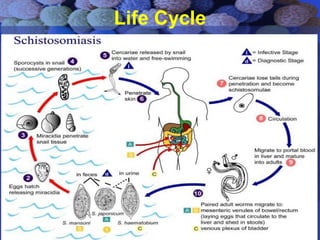
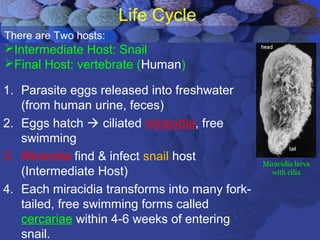
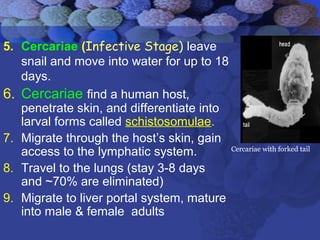
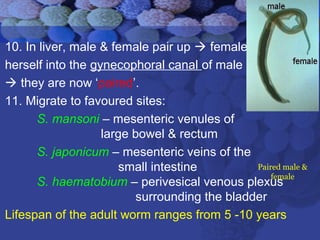
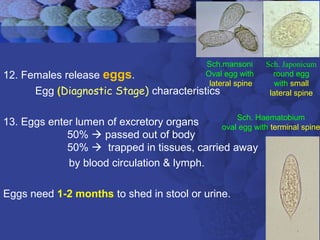
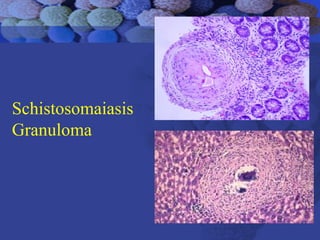
This document summarizes information about Schistosoma worms and Schistosomiasis (Bilharzia). It describes the classification, morphology, and life cycle of Schistosoma, which involves a snail intermediate host and human final host. Symptoms in humans include acute infection reactions or chronic complications in organs like the liver, intestines, bladder due to egg-induced immune responses. Diagnosis involves microscopic detection of eggs in stool/urine or other tests. Praziquantel is the primary treatment, while prevention focuses on avoiding contaminated freshwater sources.





















![Trypanosoma [1]](https://cdn.slidesharecdn.com/ss_thumbnails/trypanosomaseminar1-170312074241-thumbnail.jpg?width=640&height=640&fit=bounds)













































